
Knee Meniscus Tears

A torn meniscus is one of the most common knee injuries — about 850,000 meniscus procedures are performed in the United States every year. The meniscus is the C-shaped piece of cartilage that cushions and stabilizes your knee, and it can tear from a sudden twist on the soccer field, an awkward step down from a truck, or — in many people over 40 — simply from getting out of a deep squat. Aptiva Health treats meniscus tears at our locations in Louisville, Elizabethtown, Mount Washington, Lexington, Northern Kentucky, and Indianapolis with the full continuum of care: same-day evaluation, on-site MRI, conservative treatment, knee injections, and arthroscopic meniscus repair when surgery is needed.
Medically reviewed by J. Steve Smith, MD and the Aptiva Health Sports Medicine team — June 2026.
Torn Meniscus — The Short Version
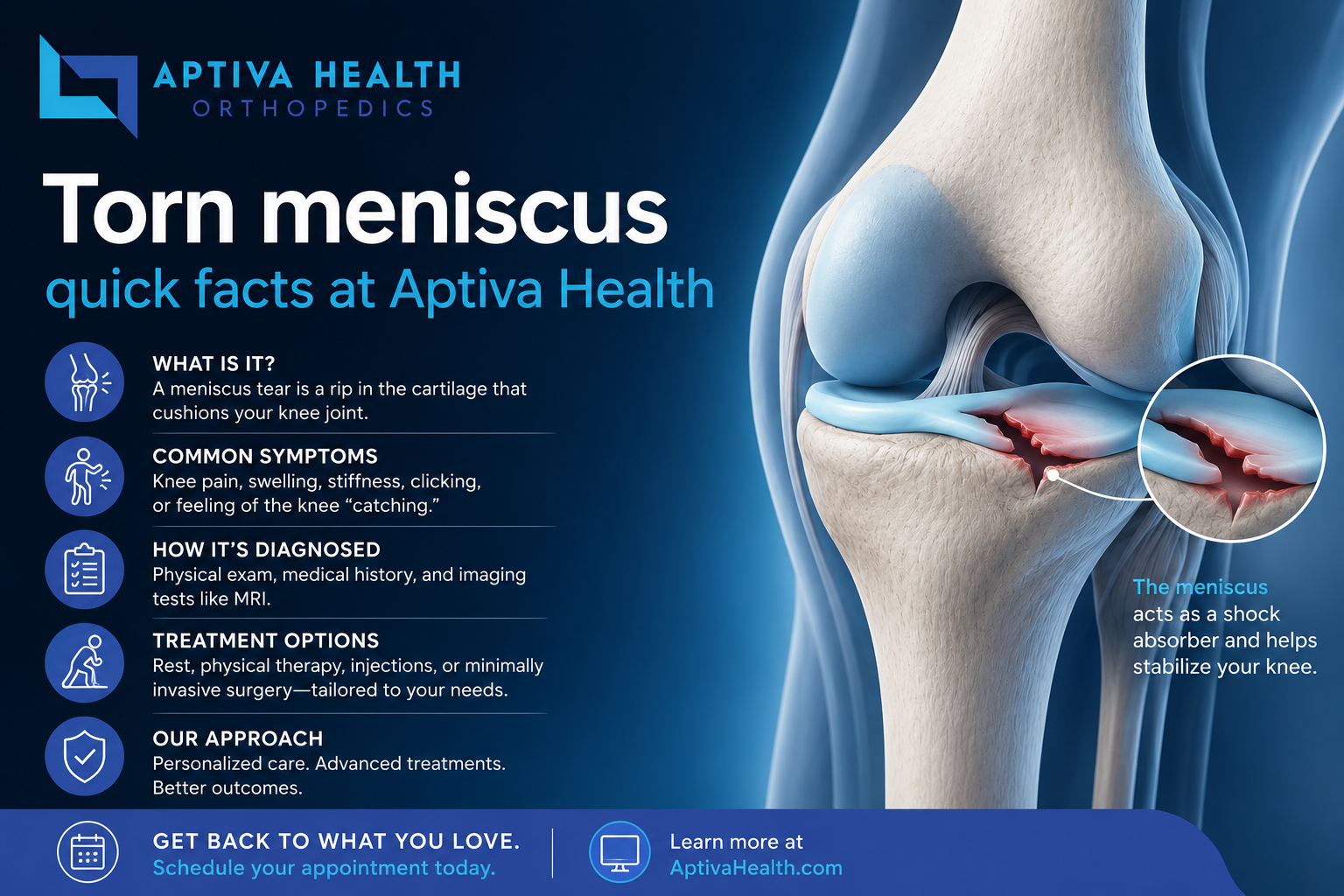
What it is: A tear in one of the two C-shaped pieces of cartilage that cushion the knee joint between the femur and tibia.
How it happens: Either suddenly (twisting injury during sports or daily activity) or gradually (degenerative wear with age, common after 40).
How it's diagnosed: Physical exam (joint line tenderness, McMurray and Thessaly tests) plus MRI.
Most common symptoms: Knee pain along the joint line, swelling, clicking or popping, catching, locking, and a sensation of the knee giving way.
Can it heal on its own? Sometimes. Tears in the outer "red zone" of the meniscus can heal because of good blood supply. Tears in the inner "white zone" usually cannot.
Does it require surgery? Not always. Many meniscus tears improve with physical therapy, anti-inflammatory medication, and time. Surgery is reserved for tears that don't respond to conservative care, mechanical locking, or active patients with repairable tears.
What Is a Knee Meniscus Tear?
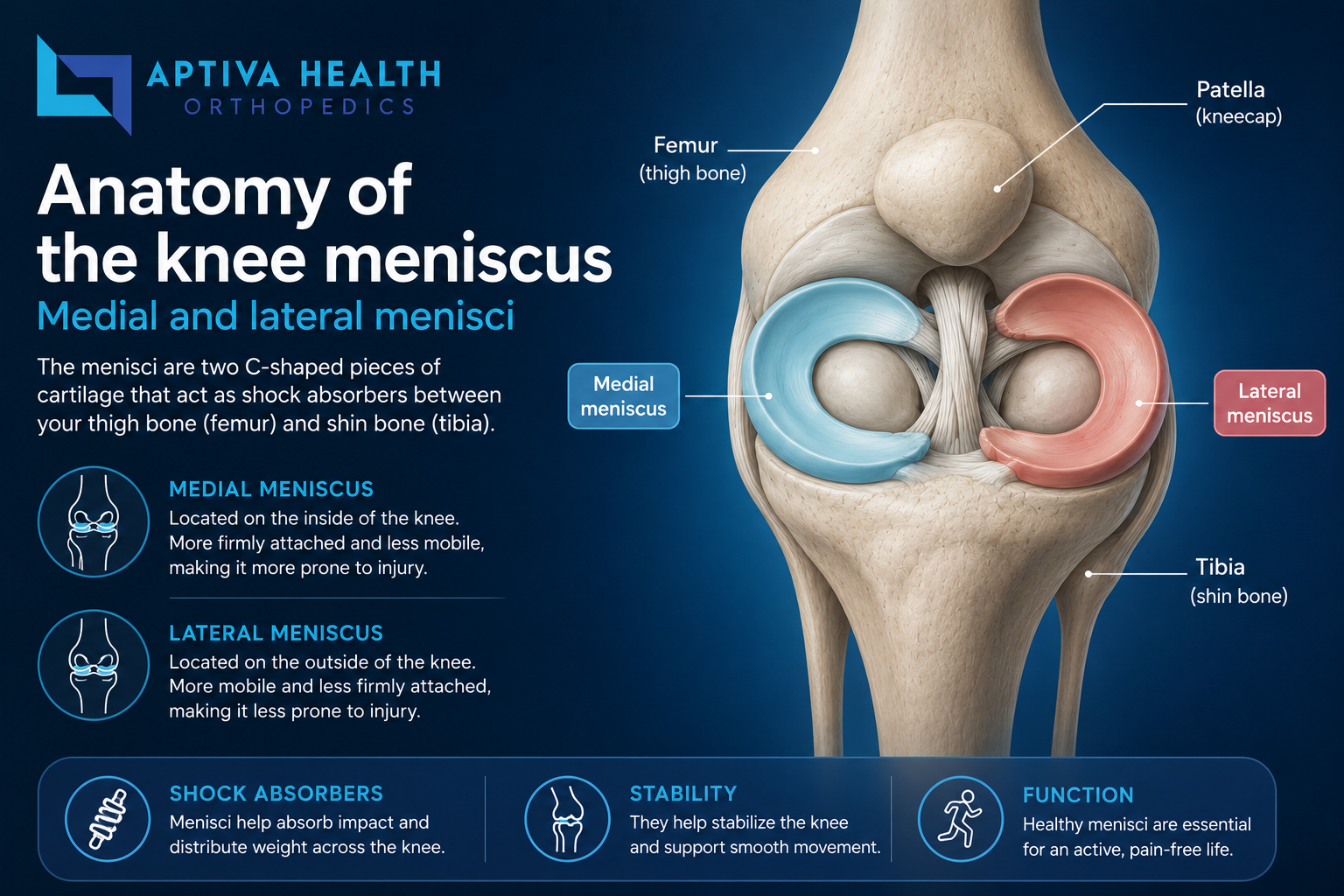
Each of your knees contains two menisci — crescent-shaped (C-shaped) pieces of tough, rubbery cartilage that sit between the bottom of your thighbone (femur) and the top of your shinbone (tibia):
The medial meniscus — on the inside of the knee
The lateral meniscus — on the outside of the knee
These pads have three critical jobs: they cushion the joint and absorb shock when you walk, run, or jump; they distribute your body weight evenly across the knee so cartilage doesn't wear out unevenly; and they help stabilize the knee.
When the meniscus tears, the smooth function of the joint is disrupted. The torn piece can flip, fold, or get caught between the bones, causing pain, catching, clicking, and sometimes mechanical locking of the knee.
Where the tear is located matters as much as the tear itself. The meniscus has three zones based on blood supply:
The outer one-third (the "red zone") has a good blood supply and can sometimes heal on its own or with surgical repair
The middle one-third (the "red-white zone") has limited blood supply
The inner two-thirds (the "white zone") has essentially no blood supply and cannot heal — torn pieces in this zone usually have to be trimmed
This is why your surgeon will often discuss tear location with you in detail: the same-size tear in two different zones requires two very different treatment approaches.

Symptoms of a Torn Meniscus
Symptoms of a torn meniscus vary depending on the size and pattern of the tear, the location, and whether the injury was sudden or gradual. The most common symptoms include:
Pain along the inside or outside of the knee at the joint line — usually worse with twisting, squatting, or going up and down stairs
Swelling that often appears 24 to 48 hours after the injury — meniscus swelling is typically delayed, unlike ACL swelling which appears within hours
Stiffness and reduced range of motion — especially difficulty fully straightening or fully bending the knee
A popping or tearing sensation at the time of injury
Clicking, snapping, or grinding during movement
Catching — a feeling that something is briefly stuck in the joint
Locking — the knee gets fully stuck in one position, usually unable to fully straighten; this is often caused by a bucket-handle tear
A sensation that the knee is giving way under load
Pain with squatting, kneeling, or twisting
Difficulty bearing weight in severe cases
If you experience a locked knee that you cannot straighten, you should be seen by an orthopedic surgeon urgently. A locked knee is one of the few meniscus tear scenarios that may require surgical attention sooner rather than later.
What Causes a Meniscus Tear?
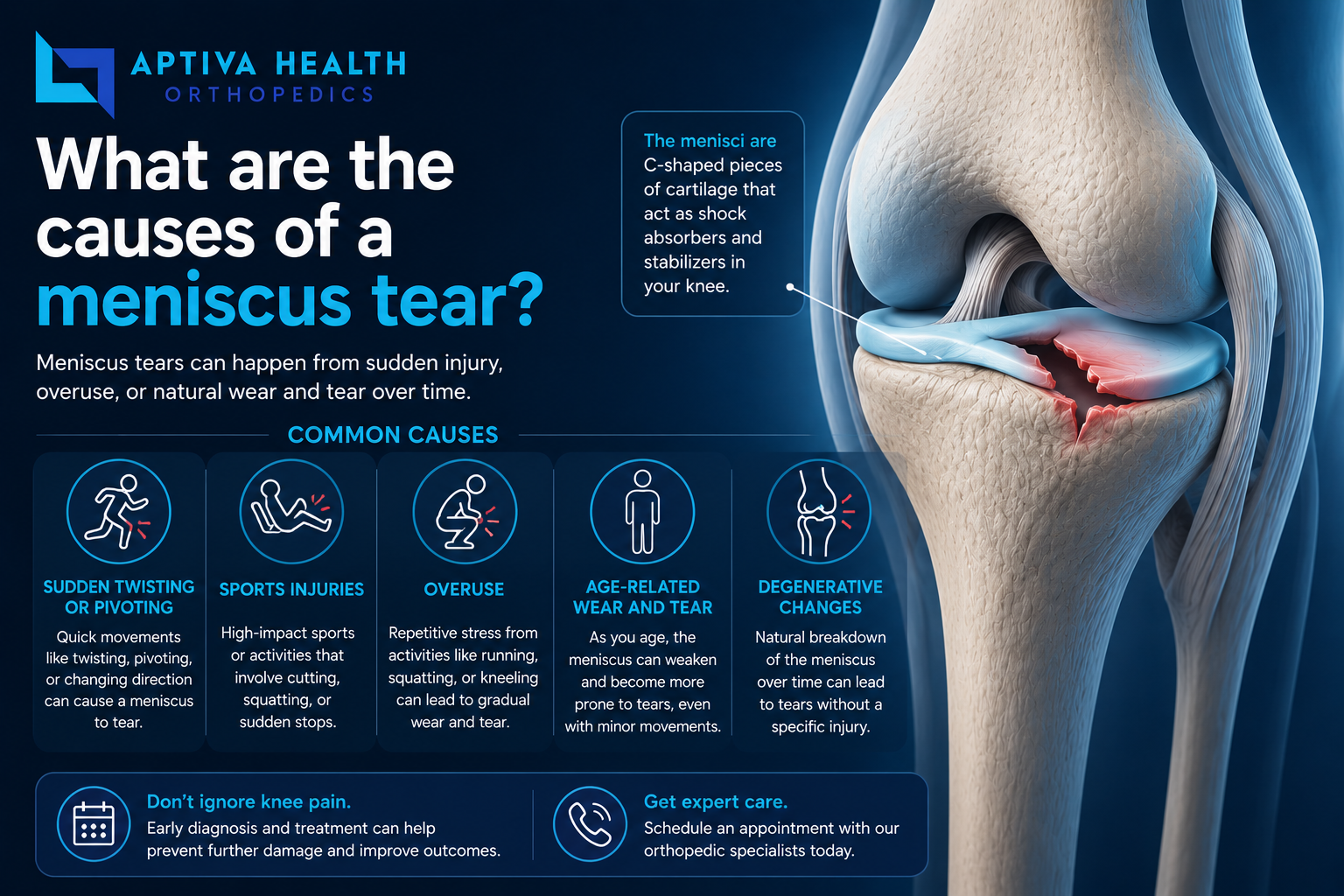
Meniscus tears fall into two broad categories — traumatic (acute injury) and degenerative (gradual wear).
Traumatic Meniscus Tears
Traumatic tears typically occur from a sudden twisting or pivoting motion of the knee while the foot is planted on the ground. Common scenarios include:
Sports — soccer, basketball, football, skiing, wrestling, tennis, and other sports involving cutting, pivoting, or contact
Work injuries — especially in occupations involving climbing, kneeling, deep squatting, or carrying heavy loads (construction, plumbing, electrical, warehousing, nursing)
Auto accidents — dashboard impact or twisting during a collision
Falls — particularly stair falls or ladder falls with a twisting component
Everyday twisting injuries — getting out of a car, lifting awkwardly, stepping down from a curb
Traumatic meniscus tears often occur together with ACL tears — roughly 40 to 50 percent of ACL tears include a meniscus injury, because the same twisting mechanism that ruptures the ACL also tears the meniscus.
Degenerative Meniscus Tears
Degenerative tears develop gradually as the meniscus weakens with age. They are very common — approximately 50 percent of adults over age 50 have evidence of a degenerative meniscus tear on MRI, though many are asymptomatic. Degenerative tears often coexist with knee osteoarthritis. The triggering "injury" can be something very minor — standing up from a deep squat, twisting to reach for something, or even no clear injury at all.
Risk Factors
Age over 40 (for degenerative tears)
Sports involving cutting, pivoting, and contact
Occupations involving deep squatting, kneeling, or climbing
Previous knee injury, especially ACL tear
Pre-existing knee arthritis
Obesity — increases mechanical load across the meniscus
Male gender — slightly higher incidence overall

How Is a Meniscus Tear Diagnosed?
Diagnosis of a meniscus tear typically combines a focused history, physical examination, and imaging.
History
Your provider will ask about how the injury happened (sudden twisting versus gradual onset), the specific location of the pain, what makes it better or worse, whether the knee has been catching, locking, or giving way, and whether you've had previous knee injuries.
Physical Examination
A thorough knee exam evaluates:
Joint line tenderness — meniscus tears almost always cause tenderness directly over the medial or lateral joint line
Range of motion — patients with meniscus tears often have a loss of full extension or full flexion
Effusion (swelling within the joint)
Provocative tests:
McMurray test — the examiner flexes the knee, then extends while rotating the leg; pain or a click suggests a meniscus tear
Apley compression test — pressing down on the heel with the knee bent reproduces pain over a meniscus tear
Thessaly test — the patient stands on one leg with the knee slightly bent and rotates the body; pain reproducing meniscus symptoms is a positive test
Ligament stability tests — to assess associated ACL, MCL, PCL, or LCL injury
Imaging
X-ray — does not show the meniscus itself but is used to rule out fracture and assess for arthritis
Magnetic resonance imaging (MRI) — the gold standard for diagnosing meniscus tears. MRI can show the tear location, pattern, and size, as well as any associated ligament or cartilage damage. Aptiva Health Imaging offers affordable on-site MRI across our locations
Diagnostic arthroscopy is occasionally used when MRI findings are unclear and surgery is being considered.
Types of Meniscus Tears
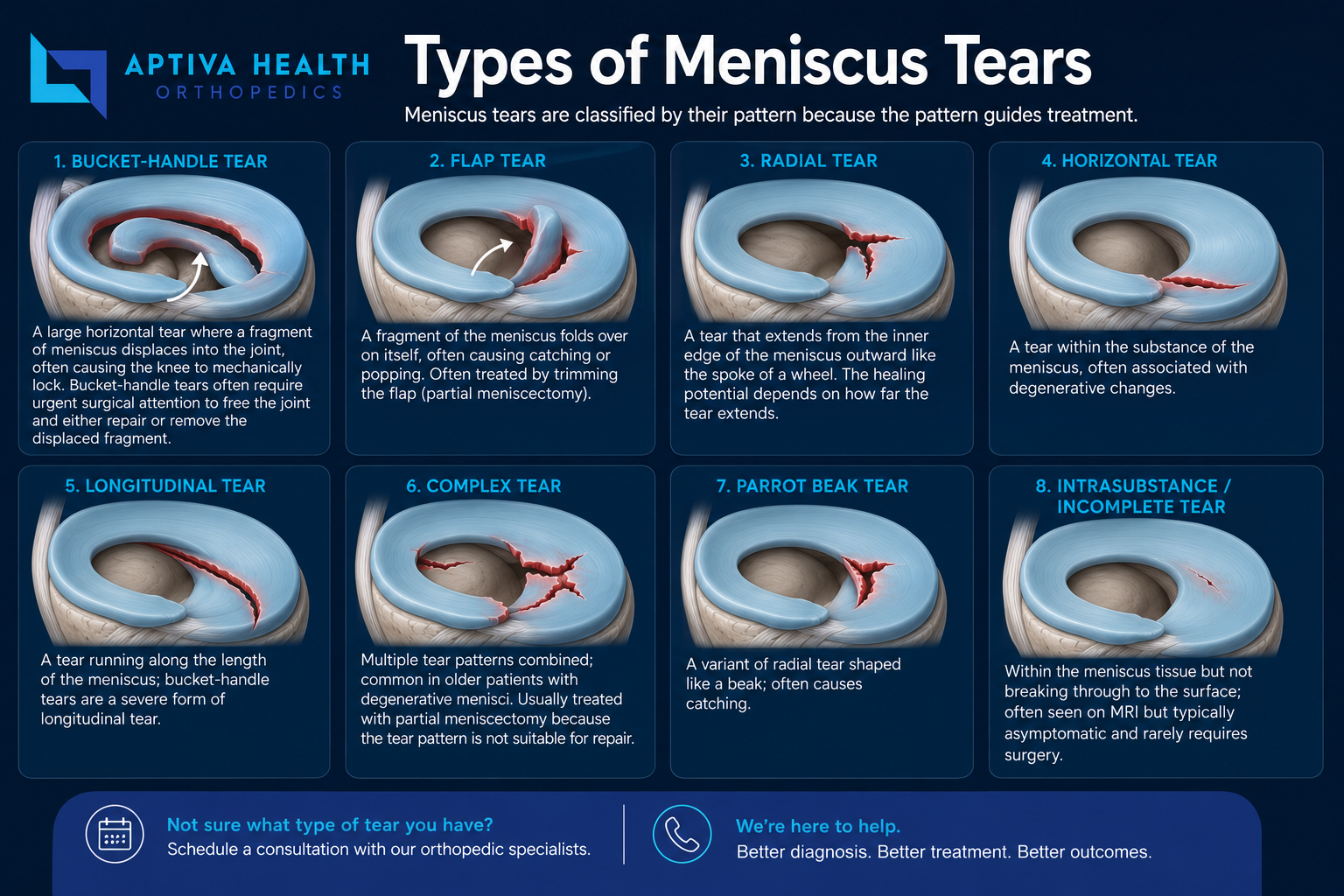
Meniscus tears are classified by their pattern because the pattern guides treatment.
Bucket-handle tear — a large horizontal tear where a fragment of meniscus displaces into the joint, often causing the knee to mechanically lock. Bucket-handle tears often require urgent surgical attention to free the joint and either repair or remove the displaced fragment.
Flap tear — a fragment of the meniscus folds over on itself, often causing catching or popping. Often treated by trimming the flap (partial meniscectomy).
Radial tear — a tear that extends from the inner edge of the meniscus outward like the spoke of a wheel. The healing potential depends on how far the tear extends.
Horizontal tear — a tear within the substance of the meniscus, often associated with degenerative changes.
Longitudinal tear — a tear running along the length of the meniscus; bucket-handle tears are a severe form of longitudinal tear.
Complex tear — multiple tear patterns combined; common in older patients with degenerative menisci. Usually treated with partial meniscectomy because the tear pattern is not suitable for repair.
Parrot beak tear — a variant of radial tear shaped like a beak; often causes catching.
Intrasubstance / incomplete tear — within the meniscus tissue but not breaking through to the surface; often seen on MRI but typically asymptomatic and rarely requires surgery.
The combination of tear pattern + tear location (red zone vs. white zone) + patient age and activity level is what determines whether your tear is best treated with physical therapy, an injection, a meniscus repair, or a partial meniscectomy.

Treatment Options for a Torn Meniscus
The right treatment depends on the tear pattern, tear location, your age and activity level, whether the knee is mechanically locking, and whether there are associated injuries (such as an ACL tear or arthritis). Treatment generally progresses through these stages.
Conservative Treatment (First-Line for Many Tears)
Rest, ice, compression, elevation (RICE) — particularly in the first days after injury
Anti-inflammatory medication — over-the-counter NSAIDs or short-term prescription options
Activity modification — avoid pivoting, squatting, and impact loading until pain improves
Bracing — a hinged knee brace or sleeve for support during recovery
Physical therapy — quadriceps strengthening, hamstring strengthening, range of motion exercises, and neuromuscular training. Often the single most effective non-surgical treatment.
Weight management — reduces mechanical load across the meniscus
Injections
When conservative care alone is not enough, knee injections can provide additional symptom relief or promote healing:
Corticosteroid injection — reduces inflammation and pain; particularly useful for degenerative tears with arthritis
Hyaluronic acid (viscosupplementation) injection — a thick fluid similar to natural joint fluid that improves lubrication; often used in older patients with associated arthritis
Platelet-rich plasma (PRP) injection — uses your body's own platelets to promote healing; emerging evidence shows benefit for meniscus tears, particularly in red-zone tears or after meniscus repair surgery
Surgical Treatment
When conservative care fails — or when the knee is mechanically locked, or in young active patients with a repairable red-zone tear — knee meniscus surgery is the next step. Aptiva Health offers the full range of arthroscopic meniscus procedures:
Arthroscopic meniscus repair — for repairable tears in the well-vascularized "red zone." The torn edges are sutured back together using small absorbable devices, preserving the meniscus. Preferred when feasible, especially in younger active patients, because the meniscus continues to protect the joint long-term.
Arthroscopic partial meniscectomy — the most common meniscus procedure. The torn portion is trimmed away through small arthroscopic incisions, removing the source of pain and mechanical symptoms while preserving as much meniscus as possible.
Meniscus transplant (meniscal allograft transplantation) — for select younger patients who have had a previous total meniscectomy and have ongoing pain without significant arthritis. A meniscus from a cadaveric donor is implanted into the knee. This is a specialized procedure reserved for specific situations.
Learn more about each procedure on our Knee Meniscus Surgery page.
Your Aptiva Health Knee Care Team
At Aptiva Health, your knee care is delivered by a multidisciplinary team of board-certified orthopedic surgeons, sports medicine specialists, advanced practice providers, and orthopedic physical therapists who care for knee patients every day — from weekend warriors to professional athletes.

Dr. J. Steve Smith — Director of Orthopedic Surgery & Sports Medicine; completed his sports medicine fellowship at the Kerlan-Jobe Orthopaedic Clinic in Los Angeles — the same program that trains team physicians for the LA Dodgers, Lakers, Kings, and Angels. Has served on the medical staffs of the Los Angeles Lakers, Los Angeles Dodgers, and Anaheim Ducks. Has performed thousands of arthroscopic knee procedures including meniscus repair and partial meniscectomy.

Dr. Timothy Wilson — Board-certified orthopedic surgeon with subspecialty certification in Sports Medicine from the American Board of Orthopaedic Surgery. More than 20 years caring for athletes across Kentucky, with past appointments as team physician for the University of Kentucky Athletics, Kentucky State University, Morehead State University, Georgetown College, and Scott County High School.

Dr. Shawn Price — Board-certified orthopedic surgeon; focuses on arthritis care and partial and total knee replacement when meniscus damage has progressed to advanced arthritis.

Dr. D. Philip Stickney — Board-certified orthopedic surgeon since 2002; treats the full range of knee conditions including meniscus tears at Aptiva's Northern Kentucky (Hebron) and Indianapolis locations.

Becky Kostyo, APRN — Orthopedic nurse practitioner. Works directly with the Aptiva Health knee team to evaluate, diagnose, and manage knee conditions including conservative care, knee injections, and pre- and post-operative coordination.

Michael Gilbert, PA-C — Orthopedic physician assistant for 30 years. Provides same-week new-patient evaluations, conservative-care coordination, knee injections, and post-operative follow-up.

Bradley Stephenson, PA-C — Orthopedic physician assistant. Provides new-patient evaluations, conservative-care coordination, knee injections, and post-operative follow-up for the Aptiva Health orthopedic and sports medicine team.

Bryan Davidson, PA-C — Orthopedic physician assistant. Treats orthopedic and sports medicine patients across the Aptiva Health network.
Physical Therapy & Imaging
Aptiva's orthopedic physical therapy, sports physical therapy, and imaging services are integrated with the knee team so your evaluation, MRI, and treatment happen under one roof.

Where We Treat Meniscus Tears
Aptiva Health treats meniscus tears and other knee injuries across our network of locations in Kentucky and Indiana. One call connects you to any of our locations: 1-844-999-3627 (DOCS).
Louisville Metro
Aptiva Health — Louisville Central — 3615 Newburg Road, Louisville, KY 40218
Aptiva Health — Louisville East — 10100 Linn Station Road, Suite 1A, Louisville, KY 40223
Aptiva Health — Louisville Downtown — 300 South 13th Street, Louisville, KY 40203
Aptiva Health — Louisville Middletown — 401 N English Station Road, Suite 1A, Louisville, KY 40223
Aptiva Health Imaging (Louisville) — 3615 Newburg Road, Suite 106, Louisville, KY 40218
Concussion & Sports Medicine Institute — 3611 Newburg Road, Louisville, KY 40218
South of Louisville
Aptiva Health — Elizabethtown — 529 Westport Road, Suite 2, Elizabethtown, KY 42701
Aptiva Health — Mount Washington — 737 N Hwy 31e Bypass, Suite 2, Mount Washington, KY 40047
Lexington / Central Kentucky
Aptiva Health — Lexington — 230 Fountain Court, Suite 180, Lexington, KY 40509
Aptiva Health Lexington MRI — 426 Codell Drive, Lexington, KY 40509
Aptiva Health Lexington Physical Therapy — 152 W Tiverton Way, Suite 180, Lexington, KY 40503
Northern Kentucky / Cincinnati Metro
Aptiva Health — Northern Kentucky — 2093 Medical Arts Drive, Hebron, KY 41048
Indianapolis
Aptiva Health — Indianapolis — 6801 Gray Road, Indianapolis, IN 46237
Main scheduling line for all locations: 1-844-999-3627 (DOCS)
Why Choose Aptiva Health for Your Knee Meniscus Tear
Sports medicine pedigree. Dr. J. Steve Smith is fellowship-trained at the Kerlan-Jobe Institute — the program that trains team physicians for the Los Angeles Dodgers, Lakers, Kings, and Angels. Dr. Timothy Wilson carries the American Board of Orthopaedic Surgery's subspecialty certification in Sports Medicine and has served as team physician for the University of Kentucky and multiple Kentucky colleges and high schools.
Conservative care first. Most meniscus tears can be managed without surgery — and even when surgery is warranted, the goal is to preserve as much meniscus as possible. We don't push surgery. We recommend the least invasive option that will get you back to your sport, your job, and your life.
Same-day and walk-in appointments. Knee injuries don't wait, and neither should you. Most patients see a sports medicine provider within days — and walk-in immediate injury care is available across our locations.
A full continuum of care under one roof. From on-site digital X-ray and MRI to physical therapy, PRP injections, and arthroscopic surgery when needed — Aptiva offers the complete knee care continuum so you don't get bounced between unrelated providers and facilities.
Multiple convenient locations. Care is available across Louisville, Elizabethtown, Mount Washington, Lexington, Northern Kentucky, and Indianapolis — close to where you live, work, and play.
Transparent insurance and cash-pay pricing. We accept most major insurance, Medicare, Medicaid Managed Care, workers' compensation, and auto insurance (PIP and Medpay). For self-pay patients, we offer transparent, bundled pricing including affordable cash-pay MRI — no surprise bills.
Schedule your appointment today!
Torn Meniscus: Frequently Asked Questions
What is a torn meniscus?
A torn meniscus is damage to one of the two C-shaped pieces of cartilage that sit between the femur (thighbone) and tibia (shinbone) in the knee joint. Each knee has two menisci — a medial meniscus on the inner side and a lateral meniscus on the outer side. They act as shock absorbers, distribute weight evenly across the joint, and help stabilize the knee. A tear can result from a sudden twisting injury during sports or daily activities, or from gradual wear and tear with age. Meniscus tears are one of the most common knee injuries, with approximately 850,000 meniscus procedures performed in the United States each year.
What are the symptoms of a torn meniscus?
The most common symptoms include pain along the inside or outside of the knee at the joint line, swelling that often appears 24 to 48 hours after the injury, stiffness and reduced range of motion, a popping or clicking sensation at the time of injury, catching or locking of the knee, and a sensation that the knee is giving way. Many patients describe difficulty fully bending or straightening the knee, especially with activities like squatting, kneeling, or going down stairs.
What does a torn meniscus feel like?
At the moment of injury, many patients describe a sharp twisting pain in the knee accompanied by a pop or tearing sensation. In the following hours to days, the knee typically becomes swollen, stiff, and painful — particularly along the joint line. Many patients report that their knee feels unreliable, with intermittent catching, locking, or giving way. With degenerative tears in older adults, the onset can be much more subtle — a gradual increase in knee pain without a clear injury.
What causes a meniscus tear?
Meniscus tears are divided into two categories. Traumatic tears typically occur from a sudden twisting or pivoting motion of the knee while the foot is planted — common in sports like soccer, basketball, football, skiing, tennis, and wrestling, but also from common movements like getting out of a car or lifting awkwardly at work. Degenerative tears develop gradually as the meniscus weakens with age, and can occur with minimal injury such as simply standing up from a deep squat. Roughly 50 percent of adults over age 50 have evidence of a degenerative meniscus tear on MRI.
Can a torn meniscus heal on its own?
Some meniscus tears can heal on their own, but most cannot. The healing potential depends primarily on its location within the meniscus. The outer one-third of the meniscus — the red zone — has a good blood supply and can sometimes heal with rest, physical therapy, and time. The inner two-thirds — the white zone — has poor blood supply and generally cannot heal on its own. Small tears in the red zone of younger patients have the highest chance of healing without surgery.
What are the different types of meniscus tears?
Meniscus tears are classified by their pattern. Common types include bucket-handle tears (a large horizontal tear where a fragment displaces into the knee, often causing the knee to lock); flap tears (a piece of meniscus folds, often causing catching); radial tears (extend from the inner edge outward); horizontal tears (within the substance of the meniscus); complex tears (multiple patterns combined); and intrasubstance or incomplete tears (within the meniscus tissue, often asymptomatic). The tear pattern, location, and patient's age and activity level determine the right treatment approach.
How is a meniscus tear diagnosed?
Diagnosis typically begins with a focused history and physical exam. Your provider will check for joint line tenderness, perform provocative tests (such as McMurray, Apley, and Thessaly tests), evaluate your range of motion, and check the stability of the knee ligaments. An X-ray is usually obtained to rule out a fracture or significant arthritis. Magnetic resonance imaging (MRI) is the gold standard for diagnosing meniscus tears and can accurately identify the tear location, pattern, and size, as well as any associated ligament or cartilage damage.
How is a torn meniscus treated?
Treatment depends on the type, location, and size of the tear, the patient's age and activity level, and whether the knee is mechanically locking. Most meniscus tears are first treated conservatively with rest, ice, compression, elevation, anti-inflammatory medication, and physical therapy focused on quadriceps strengthening and range of motion. Injections — including corticosteroid, hyaluronic acid, or platelet-rich plasma (PRP) — may be used for symptom management. Surgical treatment is considered when conservative care fails, when the knee is locked from a bucket-handle tear, or in young active patients with a repairable tear. Surgical options include arthroscopic meniscus repair (suturing the tear) or arthroscopic partial meniscectomy (trimming the damaged portion).
What is the difference between a meniscus tear and an ACL tear?
The meniscus and the ACL are two different structures in the knee, and tears of each have different symptoms. A meniscus tear is damage to the C-shaped cartilage that cushions the knee joint, and typically causes pain along the joint line, catching, locking, and clicking. An ACL tear is damage to the anterior cruciate ligament, one of the four main ligaments that stabilize the knee, and typically causes a loud pop at the moment of injury, rapid significant swelling within hours, and a sense of the knee buckling or being unstable. The two injuries often occur together — approximately 40 to 50 percent of ACL tears include a meniscus injury, because both can be caused by the same twisting mechanism.
When should I see a doctor for a possible meniscus tear?
You should see a doctor promptly if you have knee pain after a twisting injury that does not improve within a few days, persistent knee swelling, knee locking or catching, inability to fully straighten or bend the knee, knee instability or giving way, or inability to bear weight. A locked knee — meaning you cannot fully straighten it because something is mechanically blocking the joint — is one of the few meniscus tear scenarios that may require urgent surgical attention.
How long is recovery from a meniscus tear?
Recovery depends on the severity of the tear and the treatment approach. Many small tears managed conservatively with physical therapy improve significantly within four to eight weeks. After arthroscopic partial meniscectomy (trimming the torn portion), most patients return to desk work within one to two weeks, driving in one to two weeks, and full athletic activity at six to eight weeks. After arthroscopic meniscus repair (suturing the tear), recovery is longer because the meniscus needs to heal — typically four to six weeks of limited weight-bearing followed by progressive return to activity, with full sports clearance around four to six months.
Where can I get treatment for a meniscus tear near me?
Aptiva Health treats meniscus tears and other knee injuries at our locations across Kentucky and Indiana, including Louisville (Central, East, Downtown, and Middletown), Elizabethtown, Mount Washington, Lexington, Northern Kentucky (Hebron), and Indianapolis. Our sports medicine and orthopedic team includes Director of Orthopedic Surgery & Sports Medicine Dr. J. Steve Smith (Kerlan-Jobe sports medicine fellowship), board-certified orthopedic surgeons, advanced practice providers, and orthopedic physical therapists. Same-day and walk-in appointments are available. Call 1-844-999-3627 (DOCS) to schedule an evaluation at the location nearest you.
Does insurance cover meniscus tear treatment?
Yes. Treatment for meniscus tears is covered by Medicare and most major commercial insurance plans when medically necessary. Aptiva Health accepts most major insurance plans, Medicare, Medicaid Managed Care, workers' compensation, and auto insurance (PIP and Medpay). Coverage typically includes office visits, X-ray, MRI, physical therapy, knee injections, and arthroscopic meniscus surgery. Our team verifies benefits before any visit or procedure and can also provide cash-pay pricing.
