
What is Carpal Tunnel Syndrome
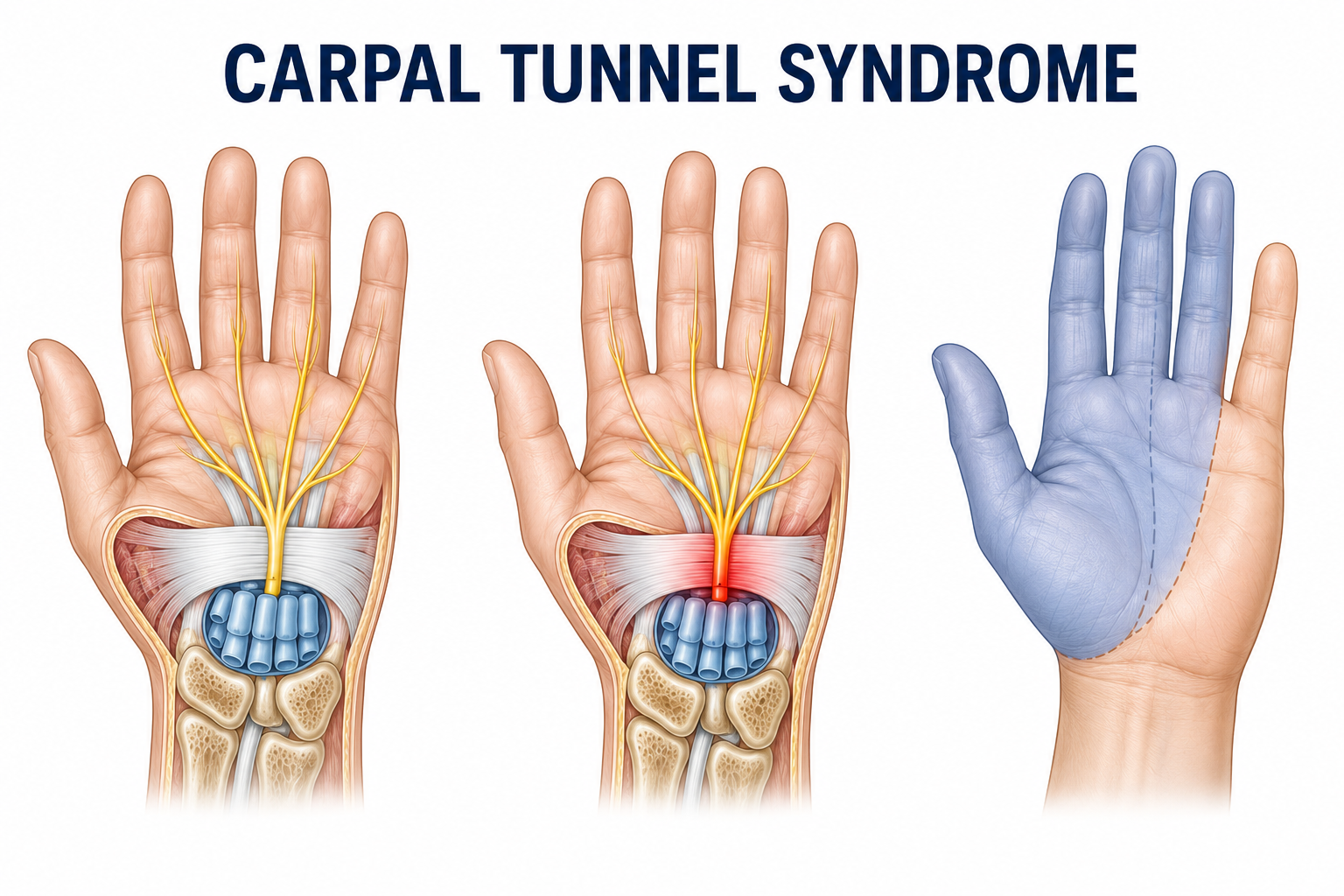
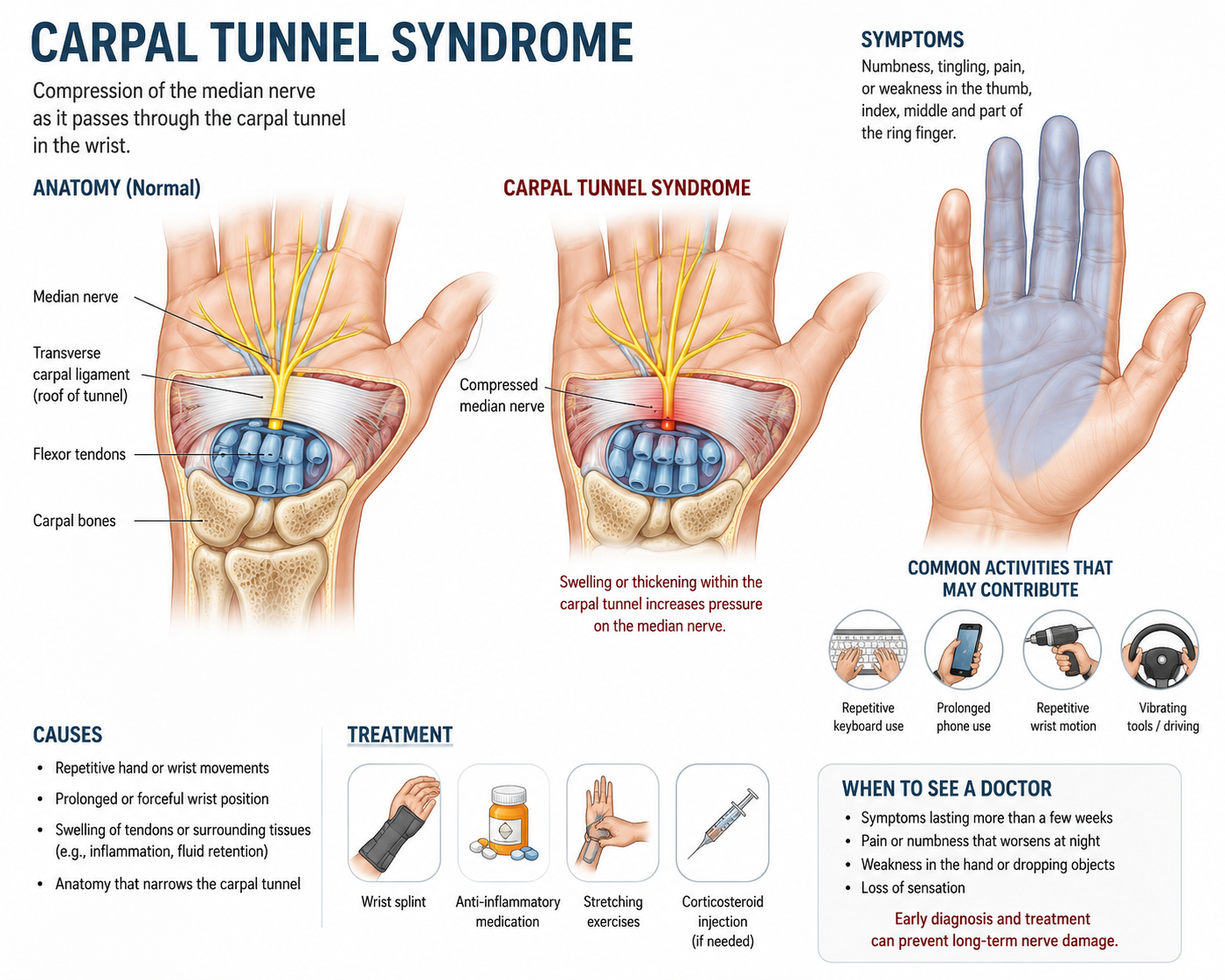
The carpal tunnel is a narrow passage on the palm side of the wrist, formed by small bones (the carpal bones) on the bottom and sides and a tough band of tissue called the transverse carpal ligament across the top. Running through that tunnel are nine tendons that bend the fingers and one critical structure: the median nerve, which carries sensation from the thumb, index finger, middle finger, and half of the ring finger — and controls some of the small muscles at the base of the thumb.
When the contents of the carpal tunnel swell — or when the tunnel itself narrows — pressure builds on the median nerve. Over time, that pressure interferes with the nerve's ability to send normal signals, producing the numbness, tingling, pain, and weakness that define carpal tunnel syndrome.
The small finger (the pinky) is typically not affected because it's served by a different nerve — the ulnar nerve. That single anatomical fact is the most reliable clue distinguishing carpal tunnel syndrome from other causes of hand numbness.
Carpal tunnel syndrome is progressive. Early symptoms tend to come and go, often appearing at night and disappearing with hand shaking. As the condition worsens, symptoms become more constant — daytime numbness, weakness, dropping objects, and eventually visible thinning (atrophy) of the muscles at the base of the thumb. Untreated severe carpal tunnel syndrome can produce permanent nerve damage that doesn't fully recover even after surgery, which is why early evaluation matters.
Medically reviewed by Timothy Wilson, MD, Shawn Price, MD, David McConda, MD, and Philip Stickney, MD - May 2026.
Schedule your appointment today!
What are common carpal tunnel symptoms?
Carpal tunnel symptoms follow a recognizable pattern. The earliest signs are usually at night, and they usually involve the same fingers in a predictable distribution.
Early-stage symptoms (often the first reported)
Nighttime numbness or tingling that wakes you up — most patients describe shaking the hand to make the symptoms go away. Many people sleep with their wrists curled, which compresses the median nerve.
Tingling in the thumb, index finger, and middle finger — sometimes the inner half of the ring finger. The pinky is almost never involved.
A "pins and needles" feeling in the hand or fingers, especially after gripping a steering wheel, phone, or book.
Hand or wrist pain that radiates up the forearm, particularly at night or after activity.
Mid-stage symptoms (as the condition progresses)
Daytime numbness or tingling that doesn't go away with hand shaking.
Decreased feeling in the fingertips — patients describe a "fuzzy" or "thick" sensation when picking things up.
Difficulty with small tasks: buttoning a shirt, gripping a steering wheel, holding a coffee cup, using a phone, typing on a keyboard.
Symptoms in both hands — carpal tunnel is bilateral in most patients, even when one side is significantly worse.
Late-stage symptoms (signs you should be evaluated soon)
Hand weakness — difficulty opening jars, gripping objects firmly, or carrying a grocery bag.
Dropping objects — especially small or smooth items like keys, pens, or coffee mugs.
Visible thinning (atrophy) of the muscles at the base of the thumb (the thenar eminence). This is a sign of long-standing nerve compression and is a strong indication for surgical evaluation.
Constant numbness that doesn't change with activity or position.
If you're experiencing thumb-side hand numbness that wakes you up at night, that's the classic textbook presentation of carpal tunnel syndrome — and it's worth getting evaluated before the symptoms become daytime, constant, or accompanied by weakness.
What causes carpal tunnel syndrome?
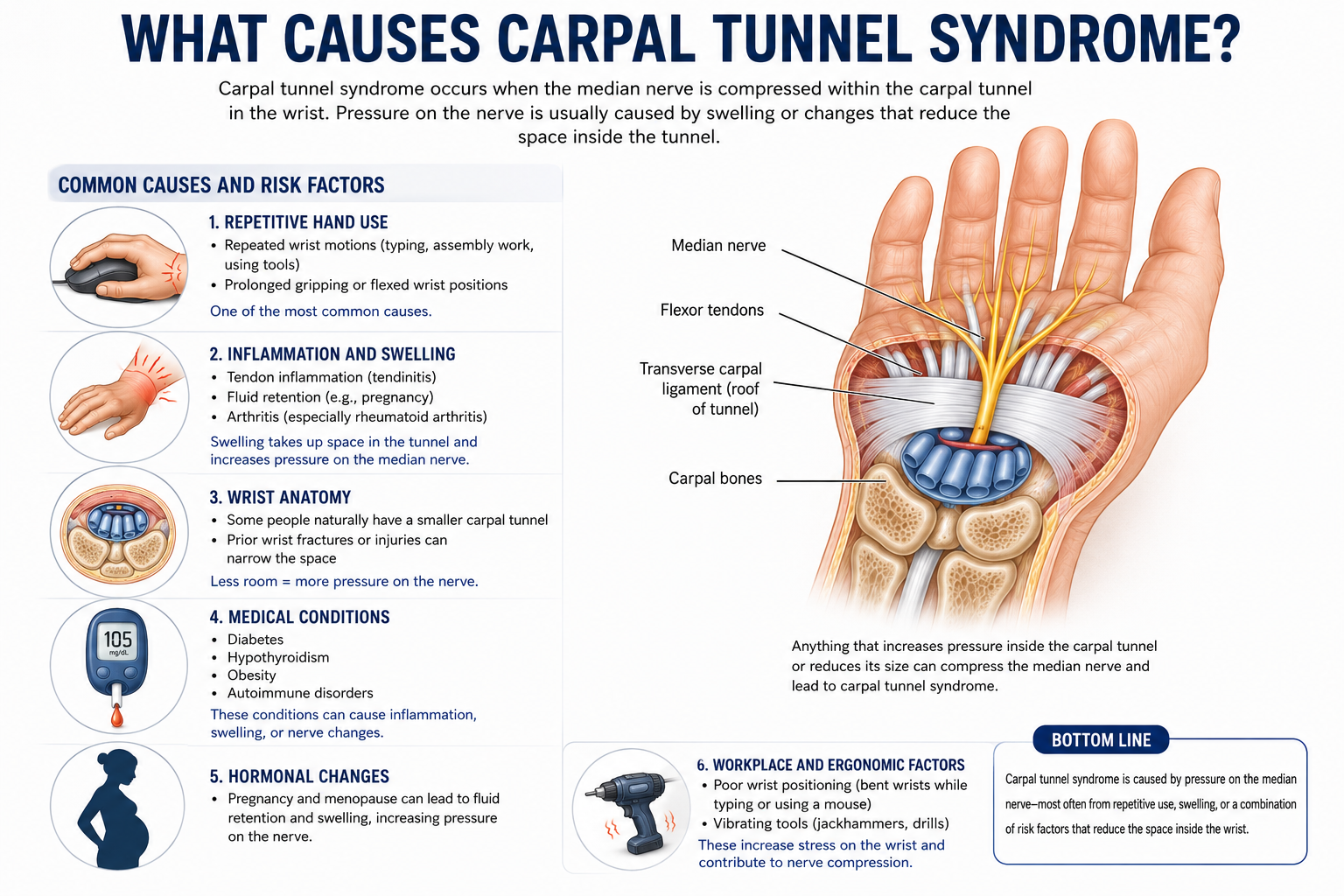
The single most common cause of carpal tunnel syndrome is anything that increases pressure inside the tunnel — either by making the tunnel smaller or by swelling its contents. Most patients have several contributing factors at once.
Anatomical factors
Smaller-than-average carpal tunnel — some people are simply born with a tighter anatomy. This is one reason carpal tunnel syndrome runs in families.
Wrist fracture or injury — prior trauma can narrow the tunnel through scar tissue or bone displacement. This includes old wrist fractures that "healed fine."
Arthritis at the wrist — bone spurs and joint changes can encroach on the tunnel.
Activity factors
Repetitive hand and wrist motion — particularly with the wrist in flexion or extension. Keyboard and mouse use, assembly line work, vibrating tool use (drills, sanders, grinders), checkout scanning, hairdressing, dental work, and meat processing are all linked to higher carpal tunnel rates. The older view that carpal tunnel is "caused by" computer use is incomplete — but repetitive forceful gripping, sustained awkward wrist postures, and vibration are well-established contributors.
Forceful or prolonged gripping — operating tools, instruments, or controls for extended periods.
Medical factors
Pregnancy — fluid retention compresses the median nerve. Pregnancy-related carpal tunnel often resolves after delivery, but some women develop chronic carpal tunnel that requires treatment.
Diabetes — diabetic peripheral neuropathy and metabolic changes both raise the risk.
Thyroid disease (especially hypothyroidism).
Rheumatoid arthritis and other inflammatory conditions.
Kidney disease and patients on dialysis.
Obesity — independently linked to higher carpal tunnel rates.
Sex and age
Women develop carpal tunnel syndrome at roughly three times the rate of men, partly because of smaller average tunnel size and partly because of hormonal factors.
Most patients are between 40 and 60 years old when symptoms become severe enough to seek care.
Carpal tunnel vs. cubital tunnel vs. cervical radiculopathy — how to tell the difference
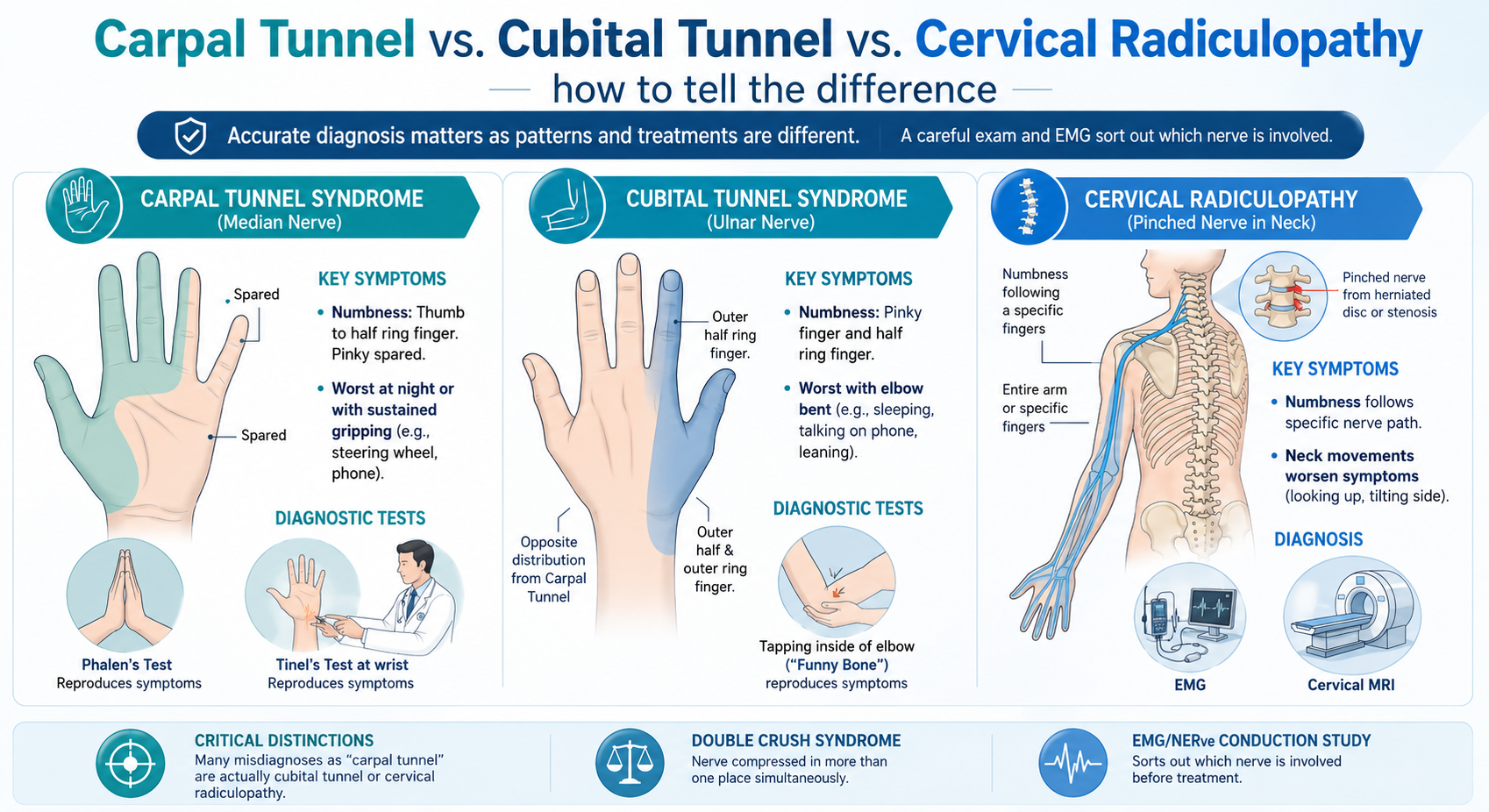
Hand numbness has several common causes, and the three most often confused are carpal tunnel syndrome, cubital tunnel syndrome, and a pinched nerve in the neck (cervical radiculopathy). Each has a different pattern, and the treatments are completely different — so accurate diagnosis matters.
Carpal tunnel syndrome affects the median nerve at the wrist. Numbness is in the thumb, index, middle, and inner half of the ring finger. The pinky is spared. Symptoms are typically worst at night and with sustained gripping (steering wheel, phone). Phalen's test and Tinel's test at the wrist reproduce the symptoms.
Cubital tunnel syndrome affects the ulnar nerve at the elbow. Numbness is in the pinky finger and the outer half of the ring finger — the opposite distribution from carpal tunnel. Symptoms are typically worst with the elbow bent for long periods (sleeping with arms folded, talking on the phone, leaning on an armrest). Tapping the inside of the elbow ("funny bone") reproduces the symptoms.
Cervical radiculopathy is a pinched nerve in the neck — typically from a herniated disc or spinal stenosis. Numbness follows the path of a specific cervical nerve root and often involves the entire arm or specific fingers depending on which level of the neck is involved. Neck movements (especially looking up or tilting to the affected side) often reproduce or worsen the symptoms. EMG and a cervical MRI confirm the diagnosis.
A surprising number of patients diagnosed with "carpal tunnel" actually have cubital tunnel or cervical radiculopathy — and a smaller number have double crush syndrome, where the nerve is compressed in more than one place at the same time. A careful exam and, when needed, an EMG/nerve conduction study sort out which nerve is actually involved before any treatment decision is made.
How is carpal tunnel syndrome diagnosed at Aptiva Health?
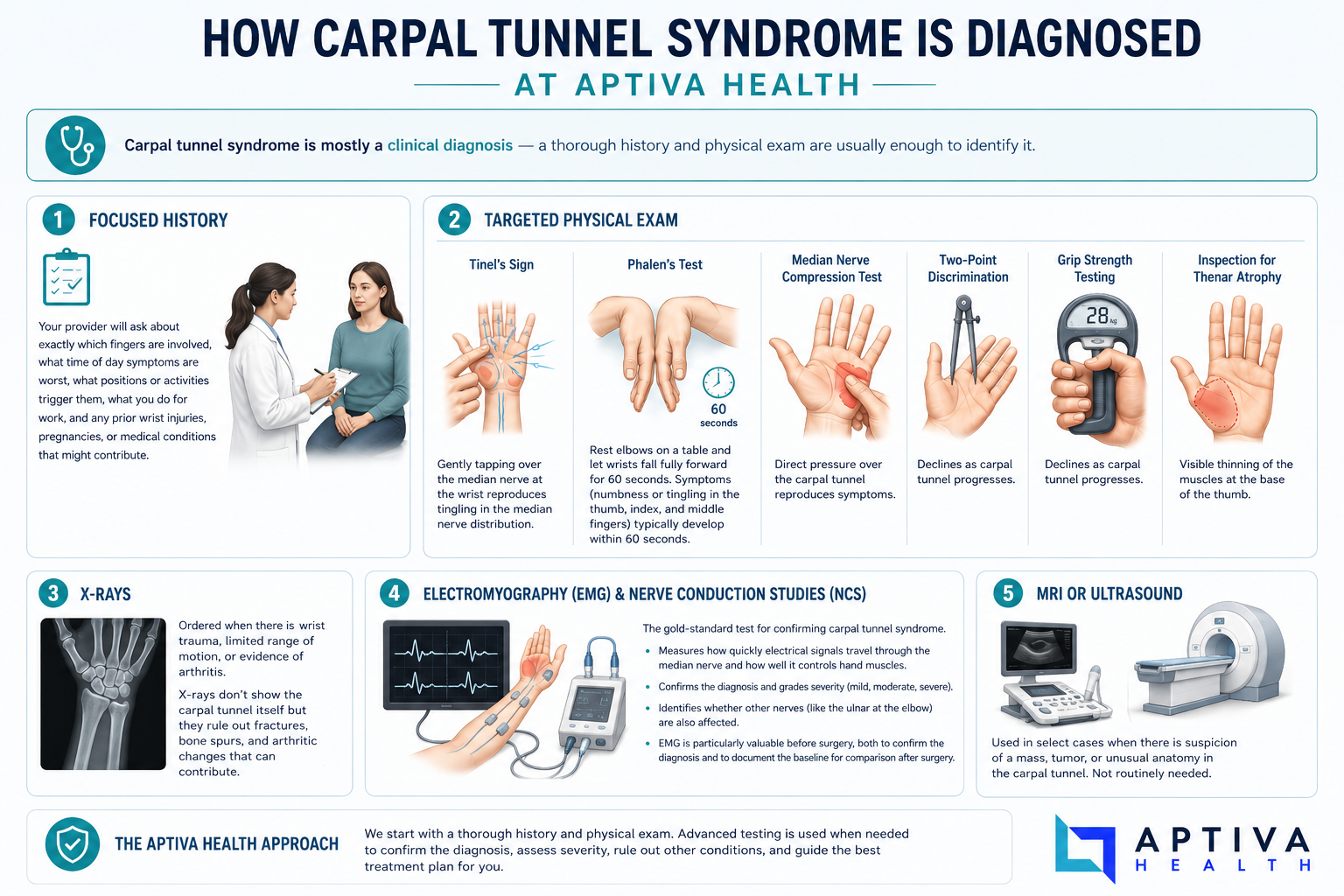
Diagnosing carpal tunnel syndrome is mostly a clinical diagnosis — a thorough history and physical exam are usually enough to identify it. At Aptiva Health, the evaluation typically includes:
A focused history. Your provider will ask about exactly which fingers are involved, what time of day symptoms are worst, what positions or activities trigger them, what you do for work, and any prior wrist injuries, pregnancies, or medical conditions that might contribute.
A targeted physical exam that includes specific provocative tests:
Tinel's sign — gently tapping over the median nerve at the wrist. A positive test reproduces tingling in the median nerve distribution.
Phalen's test — resting the elbows on a table and letting the wrists fall fully forward for 60 seconds. Patients with carpal tunnel typically develop numbness or tingling in the thumb, index, and middle fingers within 60 seconds.
Median nerve compression test — direct pressure over the carpal tunnel reproduces symptoms.
Two-point discrimination and grip strength testing — both decline as carpal tunnel progresses.
Inspection for thenar atrophy — visible thinning of the muscles at the base of the thumb.
X-rays — ordered when there is wrist trauma, limited range of motion, or evidence of arthritis. X-rays don't show the carpal tunnel itself but they rule out fractures, bone spurs, and arthritic changes that can contribute.
Electromyography (EMG) and nerve conduction studies (NCS) — the gold-standard test for confirming carpal tunnel syndrome. These tests measure how quickly electrical signals travel through the median nerve and how well it controls hand muscles. They confirm the diagnosis, grade severity (mild, moderate, severe), and identify whether other nerves (like the ulnar at the elbow) are also affected. EMG is particularly valuable before surgery, both to confirm the diagnosis and to document the baseline for comparison after surgery.
MRI or ultrasound — used in select cases when there is suspicion of a mass, tumor, or unusual anatomy in the carpal tunnel. Not routinely needed.
How is carpal tunnel syndrome treated?
Aptiva Health treats carpal tunnel syndrome with a stepped-care approach. Most patients with mild-to-moderate carpal tunnel respond well to non-surgical care. Patients with severe symptoms — particularly those with weakness, atrophy, or constant numbness — are surgical candidates from the start, because nerve damage that's allowed to progress may not recover even after surgery.
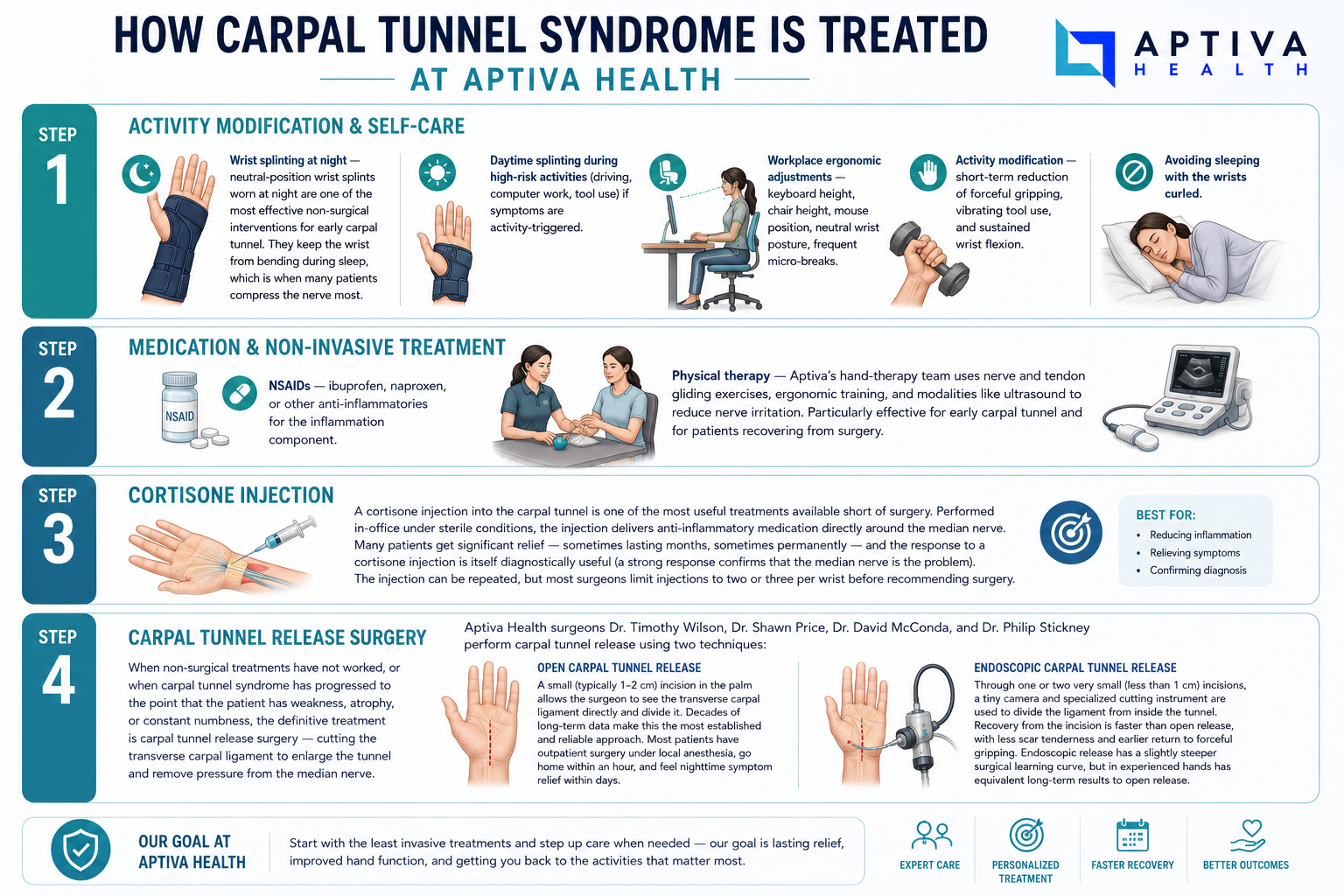
Step 1 — Activity modification & self-care
Wrist splinting at night — neutral-position wrist splints worn at night are one of the most effective non-surgical interventions for early carpal tunnel. They keep the wrist from bending during sleep, which is when many patients compress the nerve most.
Daytime splinting during high-risk activities (driving, computer work, tool use) if symptoms are activity-triggered.
Workplace ergonomic adjustments — keyboard height, chair height, mouse position, neutral wrist posture, frequent micro-breaks.
Activity modification — short-term reduction of forceful gripping, vibrating tool use, and sustained wrist flexion.
Avoiding sleeping with the wrists curled.
Step 2 — Medication & non-invasive treatment
NSAIDs — ibuprofen, naproxen, or other anti-inflammatories for the inflammation component.
Physical therapy — Aptiva's hand-therapy team uses nerve and tendon gliding exercises, ergonomic training, and modalities like ultrasound to reduce nerve irritation. Particularly effective for early carpal tunnel and for patients recovering from surgery.
Step 3 — Cortisone injection
A cortisone injection into the carpal tunnel is one of the most useful treatments available short of surgery. Performed in-office under sterile conditions, the injection delivers anti-inflammatory medication directly around the median nerve. Many patients get significant relief — sometimes lasting months, sometimes permanently — and the response to a cortisone injection is itself diagnostically useful (a strong response confirms that the median nerve is the problem). The injection can be repeated, but most surgeons limit injections to two or three per wrist before recommending surgery.
Step 4 — Carpal tunnel release surgery
When non-surgical treatments have not worked, or when carpal tunnel syndrome has progressed to the point that the patient has weakness, atrophy, or constant numbness, the definitive treatment is carpal tunnel release surgery — cutting the transverse carpal ligament to enlarge the tunnel and remove pressure from the median nerve.
Aptiva Health surgeons Dr. Timothy Wilson, Dr. Shawn Price, Dr. David McConda, and Dr. Philip Stickney perform carpal tunnel release using two techniques:
Open carpal tunnel release — a small (typically 1–2 cm) incision in the palm allows the surgeon to see the transverse carpal ligament directly and divide it. Decades of long-term data make this the most established and reliable approach. Most patients have outpatient surgery under local anesthesia, go home within an hour, and feel nighttime symptom relief within days.
Endoscopic carpal tunnel release — through one or two very small (less than 1 cm) incisions, a tiny camera and specialized cutting instrument are used to divide the ligament from inside the tunnel. Recovery from the incision is faster than open release, with less scar tenderness and earlier return to forceful gripping. Endoscopic release has a slightly steeper surgical learning curve, but in experienced hands has equivalent long-term results to open release.
Both procedures take 10–20 minutes per wrist. Most patients have outpatient surgery, return to non-strenuous activity within days, and recover full grip strength over several months. Detailed recovery expectations, including return-to-work timelines and post-op rehab, are on the carpal tunnel release surgery page.
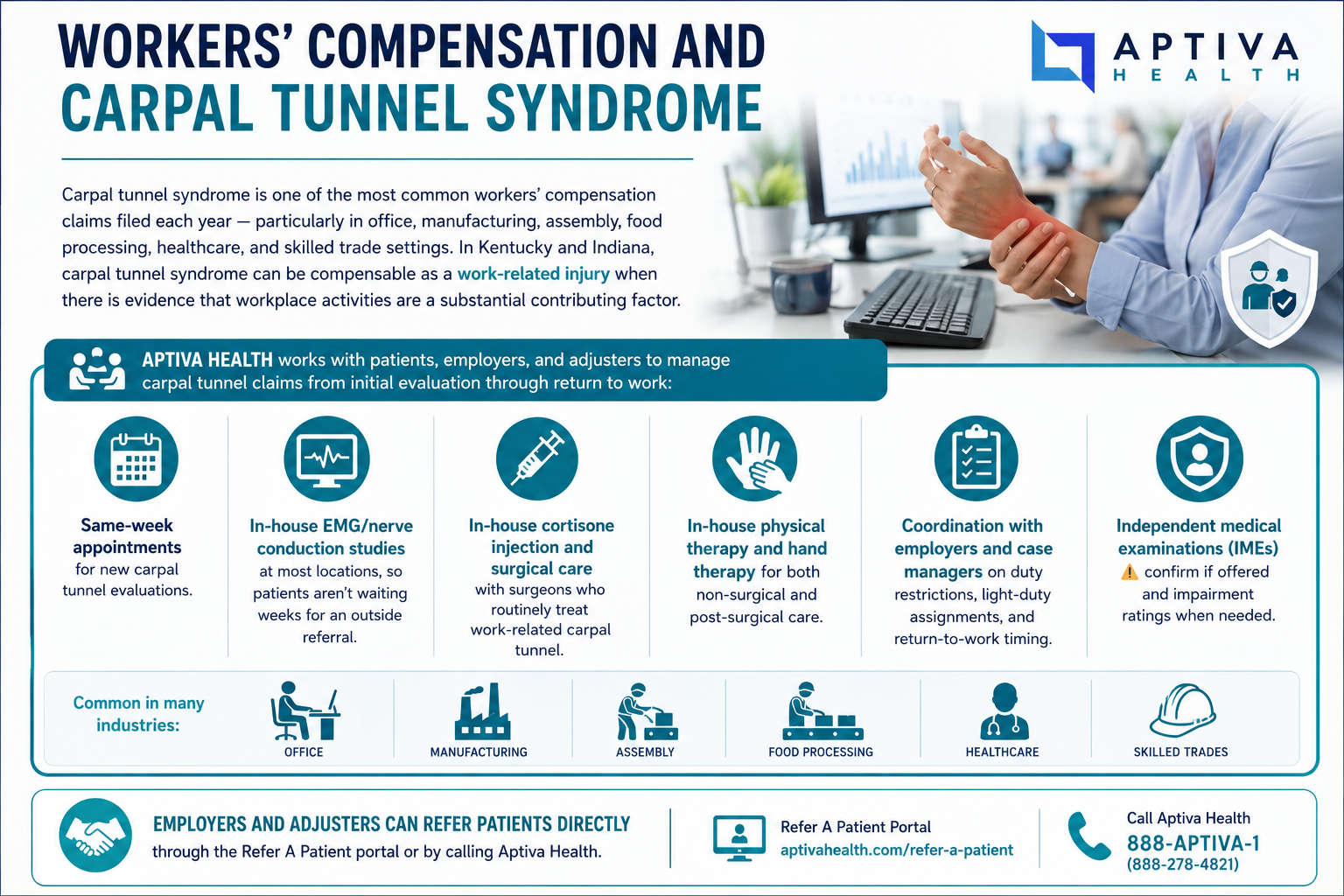
Workers' compensation and carpal tunnel syndrome
Carpal tunnel syndrome is one of the most common workers' compensation claims filed each year — particularly in office, manufacturing, assembly, food processing, healthcare, and skilled trade settings. In Kentucky and Indiana, carpal tunnel syndrome can be compensable as a work-related injury when there is evidence that workplace activities are a substantial contributing factor.
Aptiva Health works with patients, employers, and adjusters to manage carpal tunnel claims from initial evaluation through return to work:
Same-week appointments for new carpal tunnel evaluations.
In-house EMG/nerve conduction studies at most locations, so patients aren't waiting weeks for an outside referral.
In-house cortisone injection and surgical care with surgeons who routinely treat work-related carpal tunnel.
In-house physical therapy and hand therapy for both non-surgical and post-surgical care.
Coordination with employers and case managers on duty restrictions, light-duty assignments, and return-to-work timing.
Independent medical examinations (IMEs) and impairment ratings when needed.
Employers and adjusters can refer patients directly through the Refer A Patient portal or by calling Aptiva Health.

Why choose Aptiva Health for carpal tunnel treatment?
Many carpal tunnel patients end up coordinating care across three or four separate practices: a primary care office for the referral, a hand specialist for the evaluation, a separate facility for the EMG, an injection appointment somewhere else, and finally a surgery center. Aptiva Health is built differently. Every step happens under one roof:
Four fellowship-trained orthopedic surgeons who treat carpal tunnel syndrome — Dr. Timothy Wilson, Dr. Shawn Price, Dr. David McConda, and Dr. Philip Stickney — performing both open and endoscopic carpal tunnel release.
In-office cortisone injections under sterile conditions.
In-house hand therapy and physical therapy with therapists experienced in pre- and post-surgical carpal tunnel care.
Same-day and walk-in appointments at most locations.
Free 24/7 virtual access to an Aptiva orthopedic provider via the HURT! app.
Workers' compensation expertise — Aptiva routinely treats work-related carpal tunnel claims and coordinates with employers, case managers, and adjusters.
Transparent cash-pay pricing and broad in-network coverage — including Anthem, Aetna, Cigna, Humana, United Healthcare, Medicare, and most Medicaid plans.

When should you see a doctor for carpal tunnel?
Most carpal tunnel symptoms come on gradually, but certain patterns warrant prompt evaluation:
Hand numbness or tingling that wakes you up at night and is happening more than occasionally.
Symptoms that don't improve after a few weeks of wrist splinting and activity modification.
Daytime numbness that doesn't change with shaking the hand.
Dropping objects or difficulty with fine tasks like buttoning a shirt.
Visible thinning of the muscles at the base of the thumb — a sign of advanced nerve compression that needs surgical evaluation.
Carpal tunnel symptoms during pregnancy — usually managed conservatively but worth confirming the diagnosis and ruling out other causes.
Get evaluated urgently if you experience: sudden severe hand weakness, complete loss of feeling in the hand, or carpal tunnel-like symptoms following a wrist injury. These can indicate acute carpal tunnel syndrome (a rare but real surgical emergency) or another acute nerve injury.
For non-emergency carpal tunnel evaluation, Aptiva Health offers immediate orthopedic appointments at every location — patients don't need to wait weeks or months for an evaluation.
Schedule your appointment today!

We treat carpal tunnel syndrome at every Aptiva Health location!
Concussion & Sports Medicine Institute: 3611 Newburg Road, Louisville, KY 40218
Spine Center of Excellence: 3615 Newburg Road, Louisville, KY 40218
Louisville - East: 10100 Linn Station Road, Suite 1A, Louisville, KY 40223
Louisville - Downtown: 300 South 13th Street, Louisville, KY 40203
Louisville - Middletown: 401 N English Station Road, Suite 1A, Louisville, KY 40223
Lexington: 230 Fountain Court, Suite 180, Lexington, KY 40509
Lexington Physical Therapy: 152 W Tiverton Way, Suite 180, Lexington, KY 40503
Northern Kentucky: 2093 Medical Arts Drive, Hebron, KY 41048
Elizabethtown: 529 Westport Road, Suite 2, Elizabethtown, KY 42701
Mount Washington: 737 N Hwy 31e Byp, Suite 2, Mt. Washington, KY 40047
Indianapolis: 6801 Gray Road, Indianapolis, IN 46237
Frequently asked questions about carpal tunnel syndrome
How do I know if I have carpal tunnel syndrome?
The most common signs of carpal tunnel syndrome are numbness or tingling in the thumb, index, and middle fingers — often worst at night, often relieved by shaking the hand. The pinky is typically not affected. As the condition progresses, patients may notice daytime numbness, hand weakness, difficulty with small tasks, and dropped objects. A physical exam and EMG/nerve conduction study can confirm the diagnosis.
Why does my hand fall asleep at night?
Nighttime hand numbness — particularly in the thumb, index, and middle fingers — is the classic early sign of carpal tunnel syndrome. Many people sleep with their wrists curled, which compresses the median nerve and triggers symptoms. Shaking the hand often provides quick relief because it temporarily restores blood flow and reduces nerve pressure. Wrist splints worn at night are one of the most effective early treatments.
Can carpal tunnel go away on its own?
Mild, recent-onset carpal tunnel syndrome can sometimes resolve on its own, particularly when triggered by a specific activity, pregnancy, or temporary fluid retention. However, most cases of established carpal tunnel syndrome don't resolve without treatment — and untreated severe carpal tunnel can lead to permanent nerve damage. Early evaluation makes treatment more effective and protects against irreversible damage.
What's the difference between carpal tunnel and arthritis?
Carpal tunnel syndrome is caused by compression of the median nerve at the wrist — it produces numbness, tingling, and weakness, especially at night, in the thumb-side fingers. Arthritis at the wrist or hand is caused by joint inflammation and cartilage wear — it produces aching joint pain, swelling, and stiffness that's worst with use. Some patients have both conditions at the same time. The treatments are completely different, so accurate diagnosis matters.
Is carpal tunnel covered under workers' compensation?
In Kentucky and Indiana, carpal tunnel syndrome can be compensable as a work-related injury when workplace activities are a substantial contributing factor — particularly in jobs involving repetitive forceful gripping, sustained awkward wrist postures, or vibrating tool use. Aptiva Health routinely treats work-related carpal tunnel claims and coordinates with employers, case managers, and adjusters on evaluation, treatment, and return-to-work timing.
What is an EMG and do I need one?
An EMG (electromyography) and nerve conduction study measures how quickly electrical signals travel through the median nerve and how well it controls hand muscles. The test confirms the diagnosis of carpal tunnel syndrome, grades severity, and identifies whether other nerves are also affected. EMG is particularly useful before surgery and when symptoms don't fit the classic carpal tunnel pattern. Aptiva Health offers in-house EMG at most locations.
What is the difference between open and endoscopic carpal tunnel release?
Both procedures cut the transverse carpal ligament to relieve pressure on the median nerve. Open carpal tunnel release uses a small (1–2 cm) incision in the palm with direct visualization — the most established technique with decades of long-term data. Endoscopic carpal tunnel release uses one or two very small incisions and a tiny camera to divide the ligament from inside the tunnel — often allowing faster return to activity with less scar tenderness. Long-term results are equivalent. Your surgeon will recommend the approach best suited to your anatomy and symptoms.
How long is recovery after carpal tunnel surgery?
Most patients feel nighttime symptom relief within days of surgery. Stitches come out at 10–14 days. Return to non-strenuous activity (driving, light office work, daily tasks) is typically 1–2 weeks. Return to heavier activity, forceful gripping, and physical work is typically 4–6 weeks. Grip strength continues to improve for up to a year. Patients who had severe symptoms before surgery may have residual numbness that improves slowly over months or, in some cases, doesn't fully resolve.
Can I drive after carpal tunnel surgery?
Most patients can resume driving within a few days to a week after carpal tunnel release, once they can comfortably grip the steering wheel and react quickly. Surgery on the non-dominant hand allows earlier return to driving than surgery on the dominant hand. Your surgeon will give you specific guidance based on your procedure, your job, and your symptoms.
Can I have surgery on both hands at the same time?
Yes — bilateral (both-hand) carpal tunnel release is possible and is sometimes the most efficient approach for patients with severe symptoms in both hands. The trade-off is a more challenging recovery, since both hands are temporarily limited at the same time. Many patients prefer to have one hand done first, recover briefly, and then schedule the second hand. Your surgeon will help you decide which approach fits your life and your symptoms best.
How quickly can I be seen at Aptiva Health for carpal tunnel?
Aptiva Health offers same-day and walk-in orthopedic appointments at most locations across Louisville, Lexington, Northern Kentucky, Elizabethtown, Mt. Washington, and Indianapolis. The HURT! app also provides free, 24/7 virtual access to an Aptiva orthopedic provider for after-hours guidance.
Stop putting up with nighttime hand numbness and dropped objects. Aptiva Health's orthopedic team can evaluate your symptoms, perform the EMG, and start treatment — often within the same week.