
Description
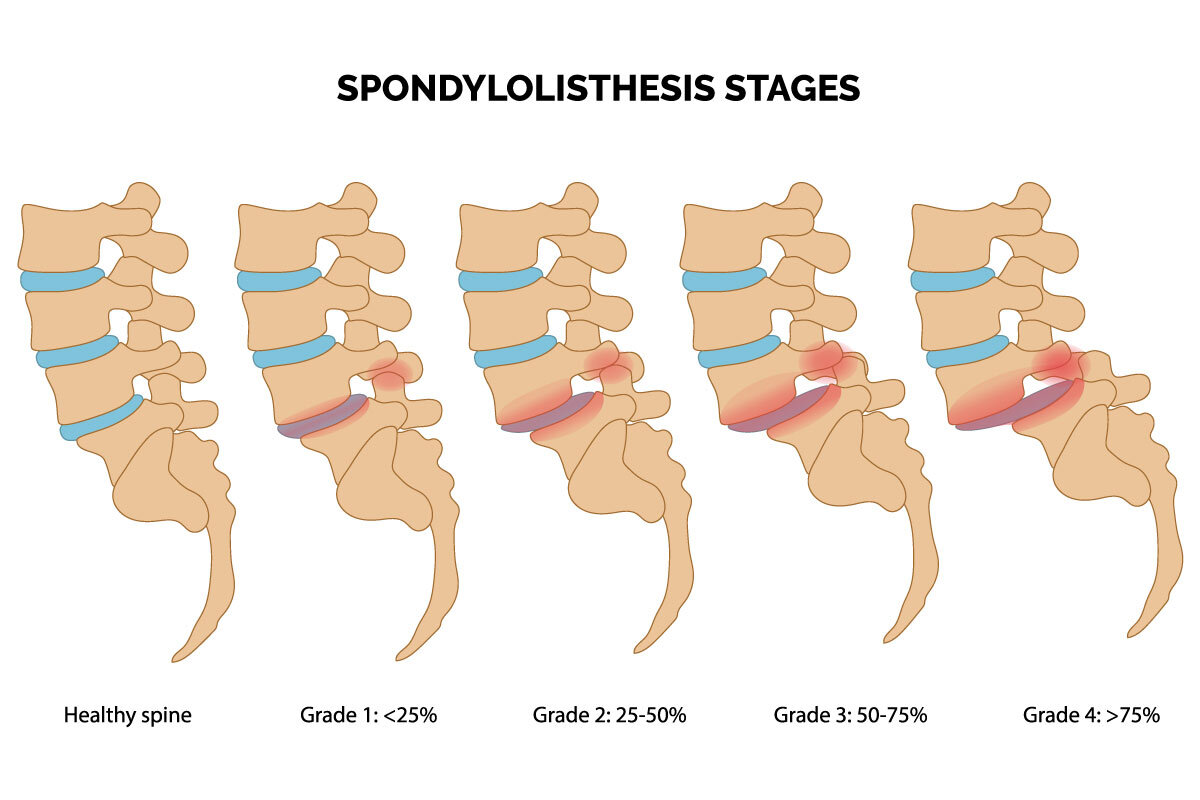
Spondylolisthesis is a condition that occurs in the low back when one of your vertebrae (the bones of your spine) slips out of place onto the vertebra below it. When the vertebrae slips out of place on the vertebra below it can cause spinal instability (which means the vertebrae move more than they should). This condition can cause the pressure on a nerve within the spine resulting in low back pain or leg pain.
At Aptiva Health, we offer same-day and walk-in appointments for spine injuries and conditions to evaluate, diagnose, and make the appropriate referral for additional treatment based upon your specific spine injury or condition. We treat spine injuries and conditions in our Spine, Pain Management, General Medicine, Orthopedics, and Physical Therapy departments.
Causes & Symptoms
Causes of spondylolisthesis vary based on age, heredity, and lifestyle. Children may suffer from this condition as the result of a birth defect or injury. However, people of all ages are susceptible if the condition is commonly exhibited within the family. Rapid growth during adolescence may also be a contributing factor to this condition.
Playing sports can also cause you to strain and overstretch, which puts stress on your lower back. The following sports have been shown to be prone to contributing to this condition:
football
gymnastics
track and field
weightlifting
Many people get Spondylolysis confused with spondylolisthesis. Both spondylolysis and spondylolisthesis cause low back pain. They are related, but not the same.
Spondylolysis: This spine defect (in its simplest form) is the formation of stress fractures or cracks within spine bones. This condition is common in young athletes.
Spondylolisthesis: This condition is when a vertebra slips out of place, resting on the bone below it. Spondylolysis may cause spondylolisthesis when a stress fracture causes the slipping or the vertebra may slip out of place due to a degenerative condition. The discs between vertebrae and the facet joints (the two back parts of each vertebrae that link the vertebrae together) can wear down. Bone of the facet joints can actually grow back and overgrow, causing an uneven and unstable surface area, which makes the vertebrae less likely to stay in place. No matter what the cause, when the vertebra slips out of place, it puts pressure on the bone below it. Some cases of spondylolisthesis do not cause symptoms. If you do feel leg pain, it can also be caused by compression or a "pinching" of the nerve roots that exit the spinal canal (the tunnel created by the interlocking vertebrae of the spine). The compression or pinching is due to the vertebrae slipping out of position and narrowing the needed space for the nerves.

symptoms
Symptoms of spondylolisthesis vary widely between patients. People with mild cases may not have any symptoms. However, those with severe cases may be unable to perform daily activities.
Some of the most common symptoms are:
Persistent lower back pain
Stiffness in your back and legs
Thigh pain
tight hamstring and buttock muscles
Difficulty walking or standing for long periods
Pain when bending over
Numbness, weakness or tingling in the foot

Diagnosis & Treatment
The most common imaging for this condition is MRI. X-rays of the affected region is typically the first imaging study conducted and often added to complete a physical evaluation of the vertebra.
X-ray: Application of radiation to produce a film or picture of a part of the body can show the structure of the vertebrae and the outline of the joints. X-rays of the spine are obtained to search for other potential causes of pain, i.e. tumors, infections, fractures, etc.
Computed tomography scan (CT or CAT scan): A diagnostic image created after a computer reads X-rays; can show the shape and size of the spinal canal, its contents and the structures around it.
Magnetic resonance imaging (MRI): A diagnostic test that produces 3D images of body structures using powerful magnets and computer technology; can show the spinal cord, nerve roots and surrounding areas as well as enlargement, degeneration and tumors.
Electromyogram and Nerve Conduction Studies (EMG/NCS): These tests measure the electrical impulse along nerve roots, peripheral nerves and muscle tissue. This will indicate whether there is ongoing nerve damage, if the nerves are in a state of healing from a past injury or whether there is another site of nerve compression. This test is ordered when the patient has pain and symptoms into the legs.
TREATMENT
Non-Surgical Treatments
The initial treatment for spondylolisthesis is usually conservative and nonsurgical in the form of rest, medications, physical therapy, bracing, and injective therapy.

Spondylolisthesis is frequently treated with nonsteroidal anti-inflammatory medication, if the pain is only mild to moderate. The spine specialist may also recommend a course of physical therapy. The physical therapist will perform an in-depth evaluation, which, combined with the doctor's diagnosis, dictates a treatment specifically designed for patients with spondylolisthesis. Therapy may include pelvic traction, gentle massage, ice and heat therapy, ultrasound, electrical muscle stimulation and stretching exercises. Pain medication and muscle relaxants may also be beneficial in conjunction with physical therapy.

An epidural steroid injection may be performed utilizing a spinal needle under X-ray guidance (through the use of a c-arm) to direct the medication to the exact level of the disc herniation for more moderate to severe symptoms.
surgery
A doctor may recommend surgery if conservative treatment options, such as physical therapy and medications, do not reduce or end the pain altogether. Doctors discuss surgical options with patients to determine the proper procedure. As with any surgery, a patient's age, overall health and other issues are taken into consideration.
The benefits of surgery should be weighed carefully against its risks. Although a large percentage of patients with spondylolisthesis report significant pain relief after surgery, there is no guarantee that surgery will help.
A patient may be considered a candidate for spinal surgery if:
Radicular pain limits normal activity or impairs quality of life
Progressive neurological deficits develop, such as leg weakness and/or numbness
Medication and physical therapy are ineffective
The patient is in reasonably good health
The patient failed interventional pain management interventions such as:
Surgery for a degenerative spondylolisthesis usually includes two parts, done together in one operation:
A decompression (also called a laminectomy)
Lumbar spine fusion with pedicle screw instrumentation
Decompression surgery (e.g. a laminectomy) alone is usually not advisable as the instability is still present and a subsequent fusion could be needed in up to 60% of patients. A 1991 randomized controlled study of fusion with and without pedicle screw instrumentation and found the fusion rates were much higher in the patients with instrumentation, but the clinical results were about the same. However, when these same patients were followed up on 10 years later, the patients with a solid fusion ultimately fared significantly better than those that had not fused.

Lumbar interbody fusion is a surgical technique that attempts to eliminate instability in the back. A MAS® TLIF achieves this by using a less invasive approach to fuse one or more vertebrae together to reduce their motion. The Aptiva Health Spine team utilizes this surgery to treat lumbar spondylolisthesis . In a MAS® TLIF procedure, rather than starting from the middle of the back and spreading the muscles to the sides like in a traditional back surgery, the MAS® TLIF approach starts off to one side of the back and splits (rather than cuts) the back muscles in one direction. This allows the surgeon to make a smaller incision with less muscle injury, which may result in less postoperative pain and a quicker recovery. This approach has proven to reduce blood loss, minimize scarring, reduce length of hospital stay, and allow for patients to recover quicker than conventional lumbar fusions. At Aptiva Health, our orthopedic spine surgeons specialize in the MAS® TLIF procedure.