
Spinal Stenosis
Spinal stenosis is a narrowing of the spaces inside the spine that puts pressure on the spinal cord or the nerves that branch out from it. It most often affects the lower back (lumbar spinal stenosis) and the neck (cervical spinal stenosis), and it is one of the most common reasons adults over 50 experience leg pain, back pain, weakness, or trouble walking. At Aptiva Health, board-certified orthopedic spine surgeons Dr. Michael Casnellie, Dr. Jaideep Chunduri, and Dr. David McConda diagnose and treat spinal stenosis with physical therapy, epidural steroid injections, the MILD procedure (minimally invasive lumbar decompression), and minimally invasive laminectomy and fusion across Louisville, Lexington, Northern Kentucky, Elizabethtown, Mt. Washington, and Indianapolis.
Medically reviewed by Michael Casnellie, MD, Jaideep Chunduri, MD, David McConda, MD, and Steven Ganzel, DO. Last reviewed: May 2026.
What is Spinal Stenosis?
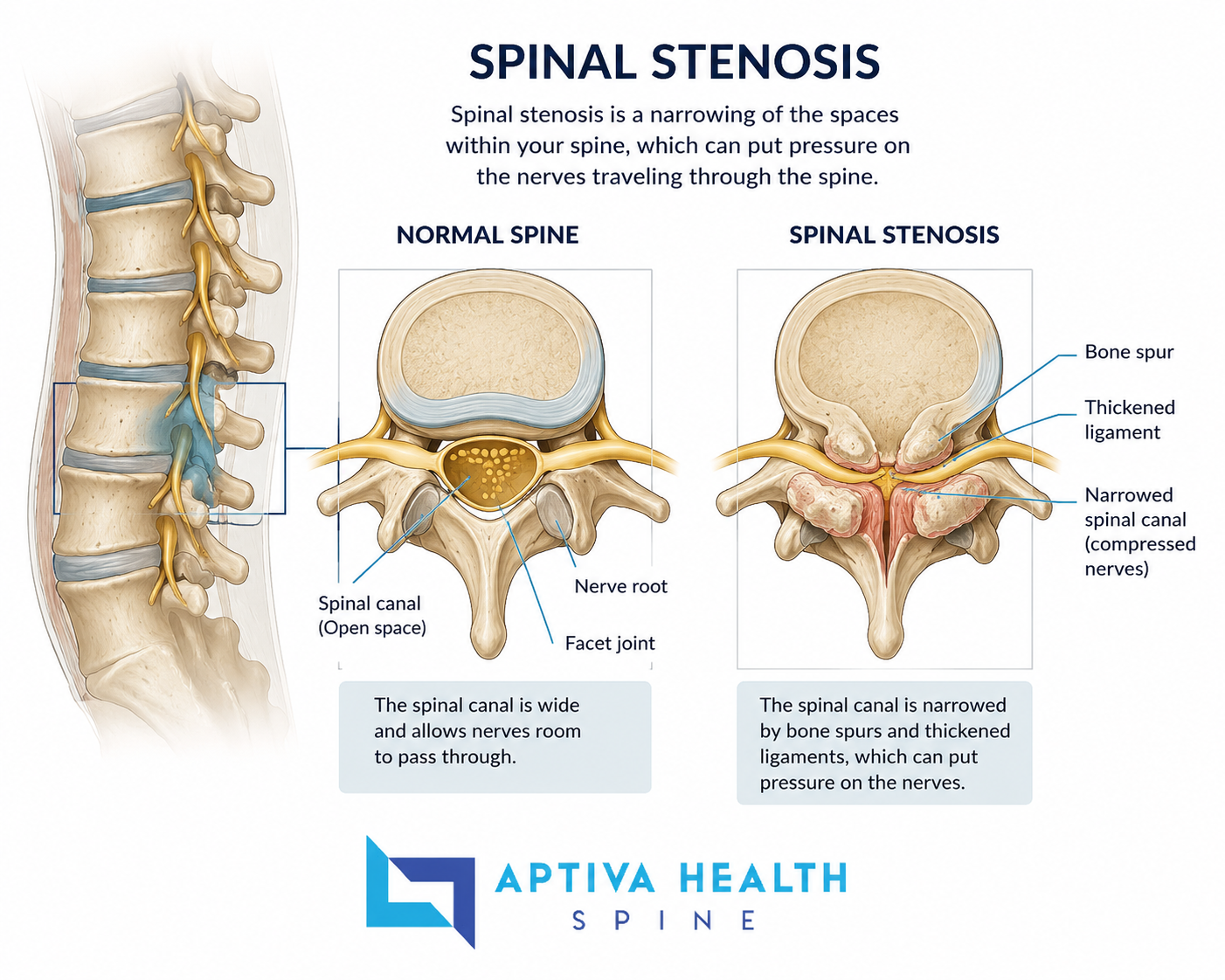
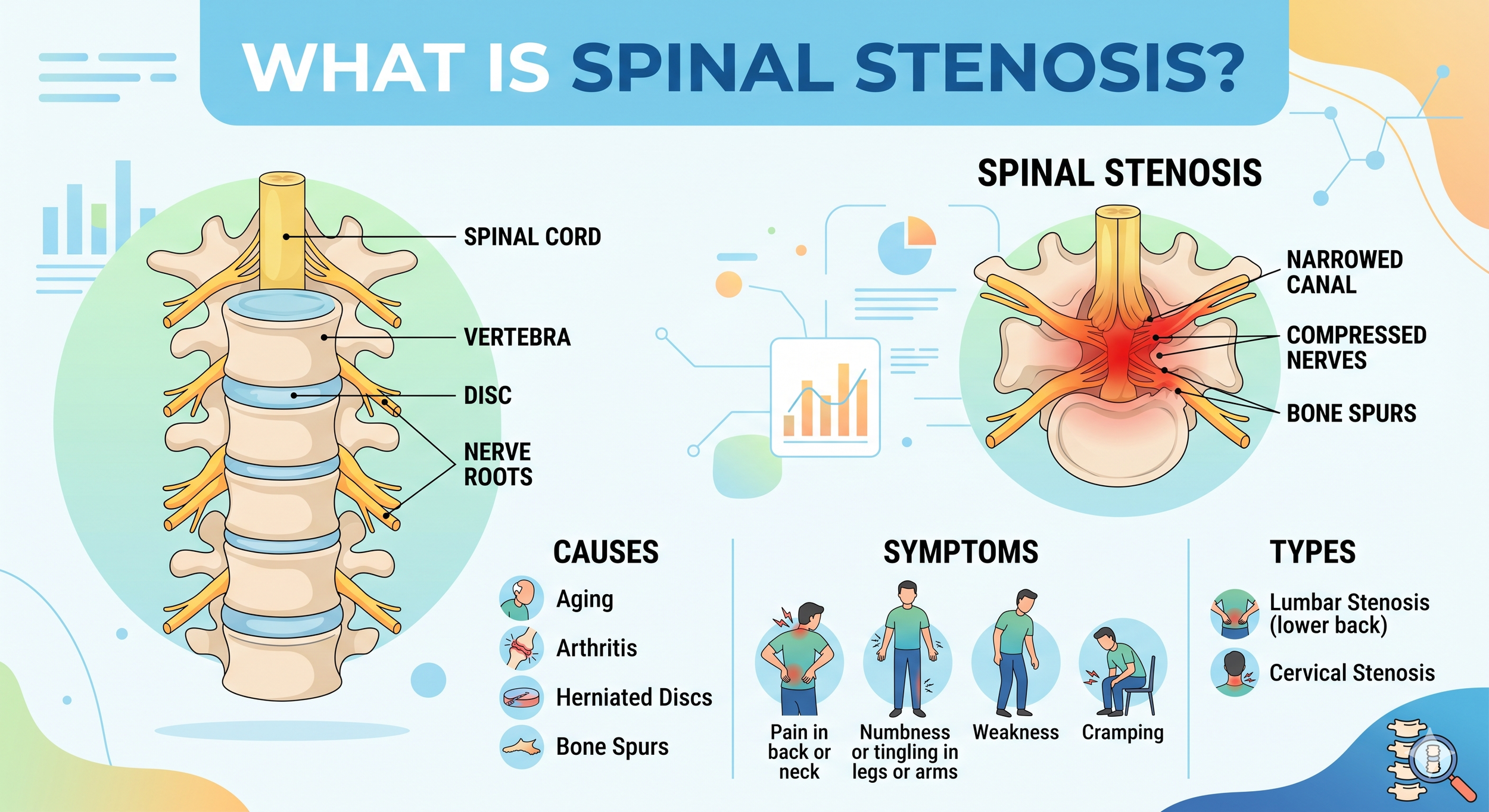
The spine is a stack of bones (vertebrae) that protects the spinal cord and the nerve roots that branch off it. Running through the center of each vertebra is a small canal — the spinal canal — that the spinal cord travels through. Smaller openings on the sides of each vertebra (the neural foramina) let individual nerve roots exit and travel out to the arms, the legs, and the rest of the body.
Spinal stenosis is the medical name for narrowing of one or both of those spaces. When the spinal canal narrows, the spinal cord itself can be compressed. When the neural foramina narrow, individual nerve roots get pinched. Either way, the result is irritation, inflammation, and over time, nerve dysfunction that produces pain, numbness, tingling, weakness, or trouble walking.
There are two main locations where spinal stenosis develops:
Lumbar spinal stenosis — narrowing in the lower back. The most common form. Affects the nerve roots that supply the legs, so symptoms usually involve back pain, buttock pain, and leg pain or weakness with walking and standing.
Cervical spinal stenosis — narrowing in the neck. Less common but potentially more serious because the spinal cord itself runs through this area. Symptoms can include neck pain, arm pain, hand clumsiness, balance problems, and — in severe cases — issues with walking, bowel, or bladder function.
Spinal stenosis is overwhelmingly an age-related condition. Most cases develop slowly over years as the spine accumulates wear-and-tear changes: discs lose height, ligaments thicken, joints develop arthritis, and bone spurs (osteophytes) form. By age 60, evidence of some degree of spinal stenosis is visible on imaging in a large percentage of adults — but only some of those people develop symptoms.
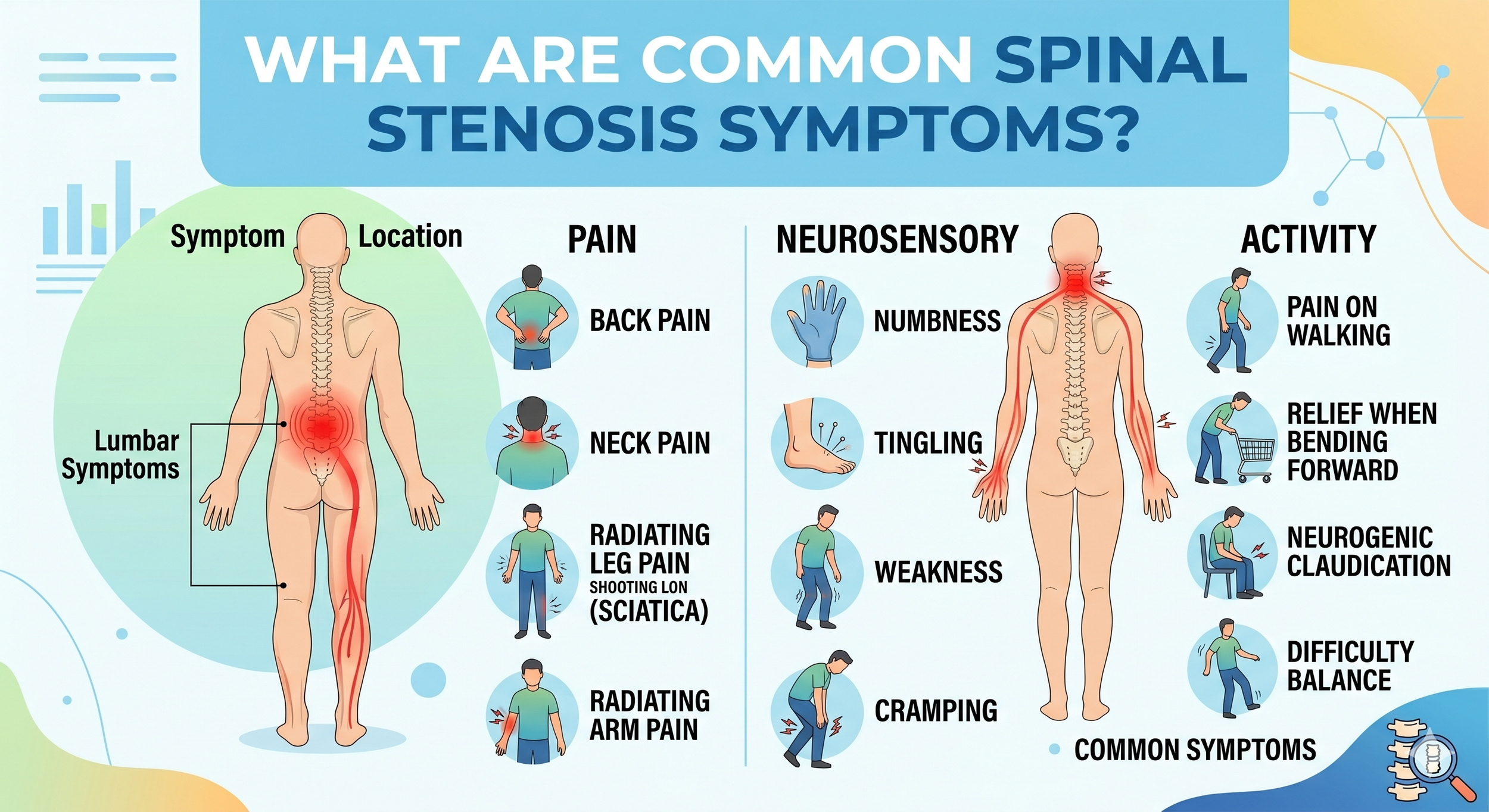
What are Common Spinal Stenosis Symptoms?
Spinal stenosis symptoms differ between cervical and lumbar stenosis, and they typically come on gradually over months or years rather than suddenly.
Lumbar spinal stenosis symptoms
Pain or cramping in one or both legs when standing or walking — often relieved by sitting down or bending forward. This pattern is called neurogenic claudication and is the hallmark of lumbar spinal stenosis.
"Shopping cart sign" — patients often notice they can walk much farther while leaning on a shopping cart, walker, or grocery cart. Bending forward opens the spinal canal slightly and takes pressure off the nerves.
Lower back pain — usually present but often less severe than the leg symptoms.
Numbness or tingling in the buttocks, legs, or feet.
Weakness in the legs — patients may notice "foot drop" or a sense that the legs feel heavy or unreliable on stairs.
Difficulty walking long distances — patients describe progressively shorter walking distances over months and years.
Symptoms that improve with sitting and worsen with prolonged standing.
Cervical spinal stenosis symptoms
Neck pain or stiffness.
Numbness or tingling in a hand or arm.
Hand clumsiness — dropping objects, trouble buttoning buttons, difficulty handwriting.
Weakness in the hand, arm, or grip strength.
Balance problems or unsteady walking — a feeling that the legs are not cooperating properly, even though the leg pain itself is not severe.
In advanced cases: bowel or bladder dysfunction, severe coordination problems, or progressive weakness — these are warning signs requiring urgent evaluation.
What Causes Spinal Stenosis?
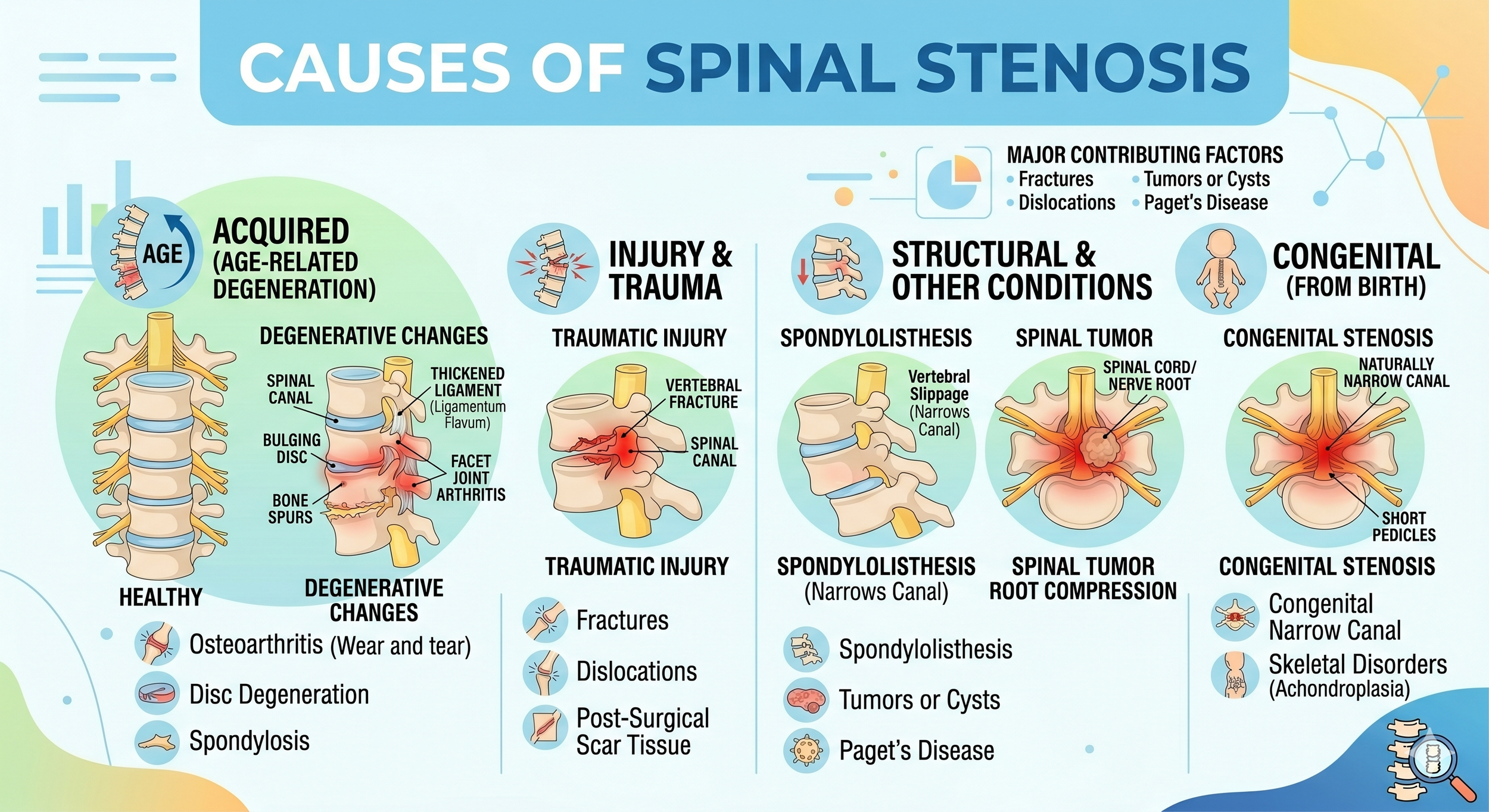
Spinal stenosis is almost always the result of gradual age-related changes that combine to narrow the spinal canal. The most common contributors are:
Bone spur (osteophyte) formation — as spinal joints develop arthritis, the body lays down extra bone around them. Those bone spurs can grow into the spinal canal or the neural foramina.
Thickened ligaments — the ligamentum flavum, a band of tissue at the back of the spinal canal, naturally thickens with age. In some patients it becomes thick enough to compress the canal on its own. This is one of the changes the MILD procedure is specifically designed to treat.
Disc bulges and herniations — discs lose height and water content with age, and the disc material can bulge backward into the canal.
Degenerative spondylolisthesis — when wear-and-tear changes allow one vertebra to slip forward over the one below it, the spinal canal narrows at that level. Common at L4–L5.
Spinal injuries — fractures, dislocations, or post-surgical scar tissue can narrow the canal.
Congenital factors — some people are born with a smaller-than-average spinal canal. These patients develop symptoms earlier in life when age-related changes start adding up.
Less commonly: tumors, bone diseases such as Paget's disease, and inflammatory conditions.
Most patients with spinal stenosis have more than one of these factors contributing at the same time, which is why a thorough evaluation by a spine specialist matters before deciding on a treatment plan.
How is Spinal Stenosis Diagnosed at Aptiva Health?
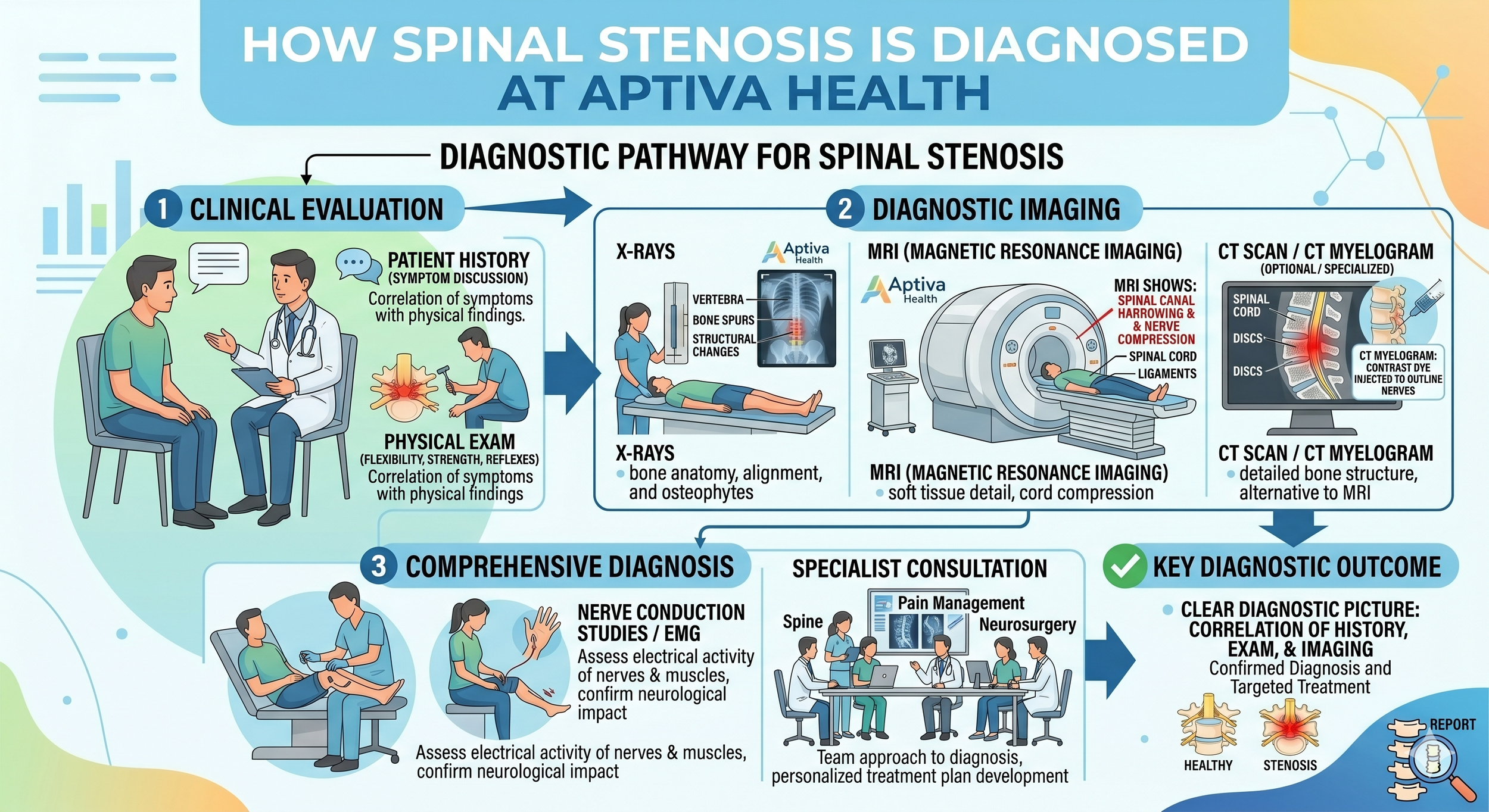
Diagnosing spinal stenosis is as much about ruling out other causes of similar symptoms as it is about confirming the spinal anatomy. At Aptiva Health, your evaluation typically includes:
A detailed medical history. Your provider will ask about exactly where the pain or weakness is, what makes it better or worse, how far you can walk before symptoms start, whether you get relief from leaning forward or sitting, and any history of back surgeries, falls, or progressive symptoms.
A focused neurologic exam. This includes reflex testing, strength testing of specific muscle groups, sensation testing, and balance assessment. The pattern of which nerves are involved often points to exactly where in the spine the stenosis is.
Imaging. Two imaging studies are used together to confirm spinal stenosis:
X-ray — shows bony alignment, bone spurs, disc-space narrowing, and any vertebral slippage (spondylolisthesis). Fast and inexpensive; usually the first study ordered.
Magnetic resonance imaging (MRI) — the most accurate study for spinal stenosis because it shows the soft tissues (discs, ligaments, spinal cord, nerve roots) along with the bones. MRI can show exactly which nerves are compressed and by what. Aptiva Health operates its own MRI imaging centers, so most patients can get same-week scheduling.
CT or CT myelogram — used when MRI is not possible (pacemakers, certain implants) or when bony detail needs to be clearer than MRI provides.
Rule out non-spine causes. Leg pain with walking is the classic symptom of lumbar spinal stenosis — but it can also be caused by peripheral arterial disease (PAD), hip arthritis, or peripheral neuropathy. A good spine evaluation distinguishes between these because the treatments are completely different.
Spinal Stenosis vs. Herniated Disc vs. Peripheral Arterial Disease — How to Tell the Difference
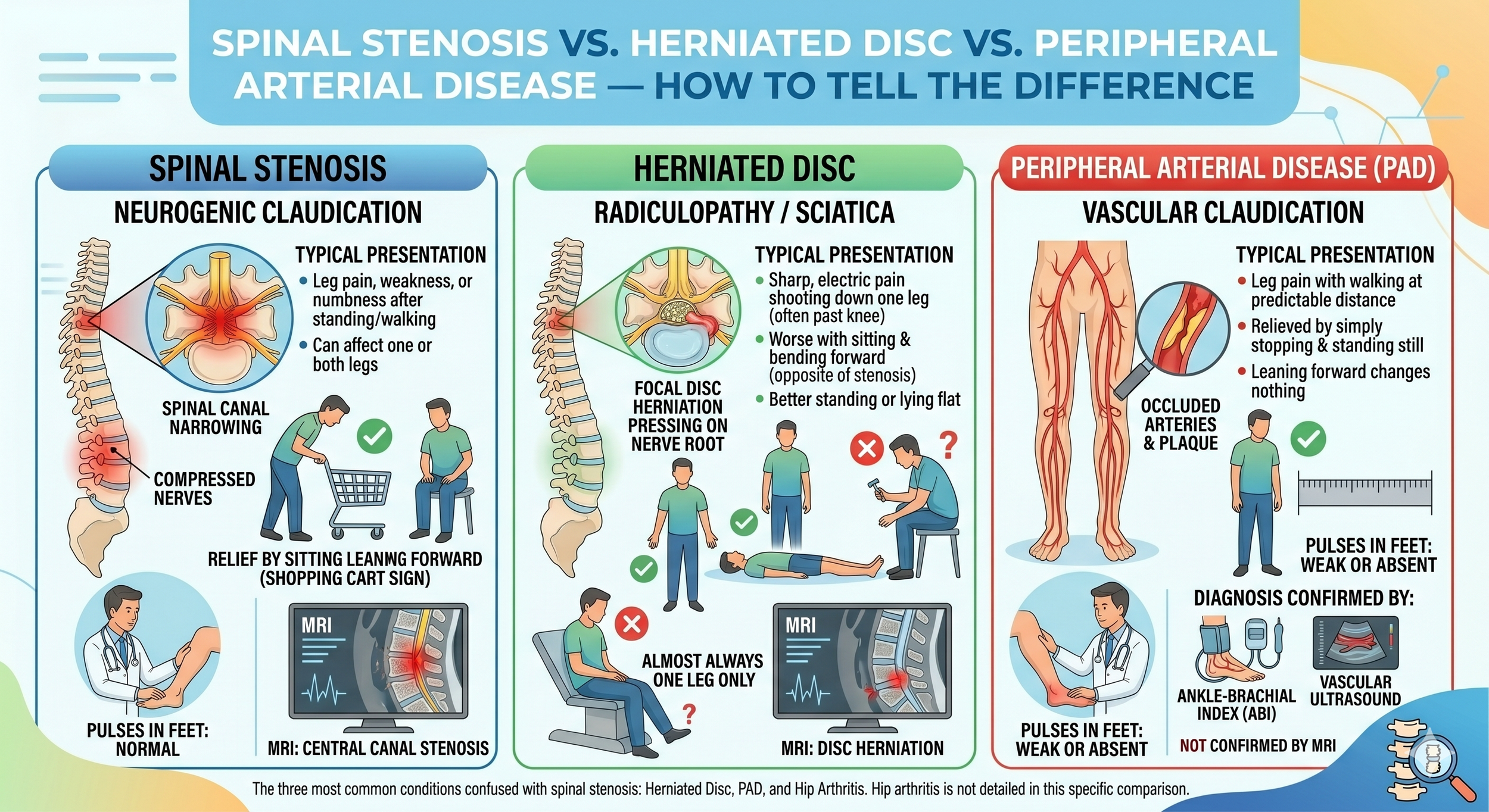
The three most common conditions confused with spinal stenosis are a herniated disc, peripheral arterial disease (PAD), and hip arthritis. Each has a different pattern.
Spinal stenosis (neurogenic claudication) typically causes leg pain, weakness, or numbness that starts after standing or walking for a while. The pain is relieved by sitting or leaning forward (the shopping cart sign). It can affect one or both legs. Pulses in the feet are normal. MRI shows narrowing of the spinal canal.
Herniated disc (radiculopathy / sciatica) typically causes sharp, electric pain shooting from the lower back down one leg, often past the knee. The pain is usually worse with sitting and bending forward, and better when standing or lying flat — the opposite pattern from spinal stenosis. It almost always affects one leg only. MRI shows a focal disc herniation pressing on a nerve root.
Peripheral arterial disease (PAD) (vascular claudication) also causes leg pain with walking, but the pain comes on at a fairly predictable distance and is relieved by simply stopping and standing still — leaning forward does not change anything. Pulses in the feet are weak or absent. The diagnosis is confirmed by an ankle-brachial index (ABI) or vascular ultrasound, not an MRI.
Hip arthritis causes groin, buttock, or thigh pain that often gets worse with walking but rarely radiates below the knee. It usually responds to a hip injection and is confirmed by hip X-ray and exam.
Many older patients have more than one of these conditions at the same time, which is why a careful evaluation by a fellowship-trained spine team is the most reliable way to identify everything that is contributing to the symptoms — and to sequence treatment correctly.

How is Spinal Stenosis Treated at Aptiva Health?
Aptiva Health treats spinal stenosis with a stepped-care approach. Most patients get meaningful relief from non-surgical care. Patients who do not respond after several months of conservative treatment, or whose anatomy clearly will not improve without decompression, are candidates for the MILD procedure or surgery.
Step 1 — Activity modification, medication & self-care
Activity modification — short-term avoidance of the postures and activities that aggravate symptoms (typically prolonged standing or walking long distances), combined with the postures that relieve them (sitting, leaning forward, riding a stationary bike).
NSAIDs — ibuprofen, naproxen, or other anti-inflammatories to reduce nerve-root inflammation.
Acetaminophen — for patients who can't tolerate NSAIDs.
Anti-seizure medications for nerve pain — gabapentin (Neurontin) and pregabalin (Lyrica) are commonly prescribed for the nerve-pain component of spinal stenosis.
Short courses of muscle relaxants — for the muscle-spasm component that often accompanies stenosis.
Heat and cold therapy — alternating ice and heat at home.

Step 2 — Physical therapy & non-invasive treatments
Physical therapy — Aptiva's in-house physical therapy team uses spinal stenosis-specific protocols focused on flexion-based exercises (because flexion opens the spinal canal), core and gluteal strengthening, and gait training. Aquatic therapy is particularly effective for spinal stenosis because the buoyancy unloads the spine.
Dry needling — for the muscle component of the pain.
TENS (transcutaneous electrical nerve stimulation) — wearable battery-powered device that may reduce pain perception.
Bracing — a flexion-biased lumbar brace can be helpful in select cases.
Step 3 — Interventional pain management injections
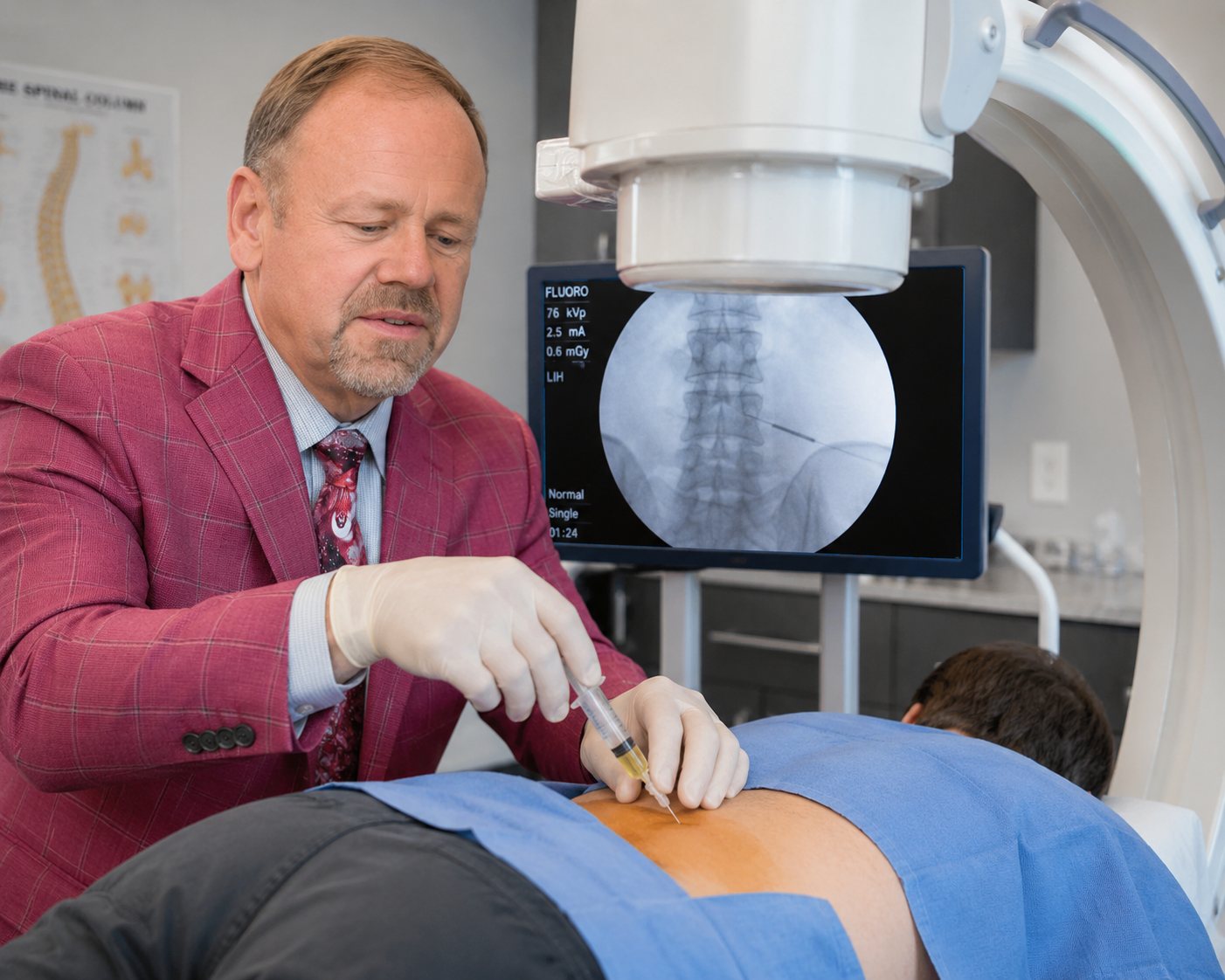
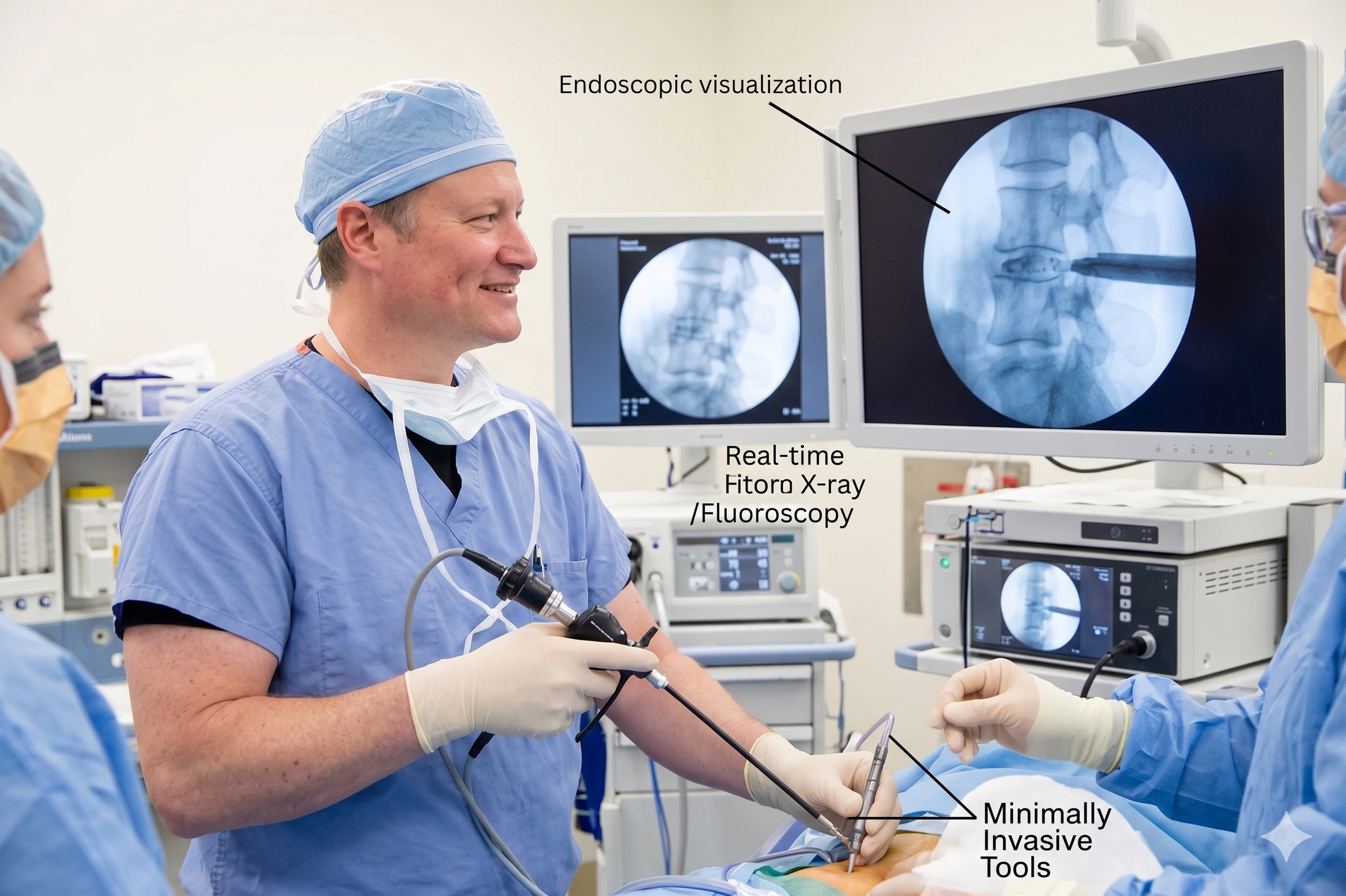
When physical therapy and oral medication aren't enough, Dr. Steven Ganzel — Aptiva's double board-certified pain management physician — performs targeted injections under fluoroscopic (live X-ray) guidance:
Lumbar epidural steroid injection — anti-inflammatory medication delivered directly into the epidural space around the inflamed nerve roots. Often provides significant relief that lets the patient fully engage with physical therapy.
Facet joint injection — when the small joints between vertebrae are contributing to the pain.
Medial branch block — diagnostic injection to confirm facet-joint involvement before radiofrequency ablation.
Radiofrequency ablation (rhizotomy) — for facet-joint pain that responds to a medial branch block; can provide six to twelve months of relief.
Step 4 — The MILD procedure (Minimally Invasive Lumbar Decompression)
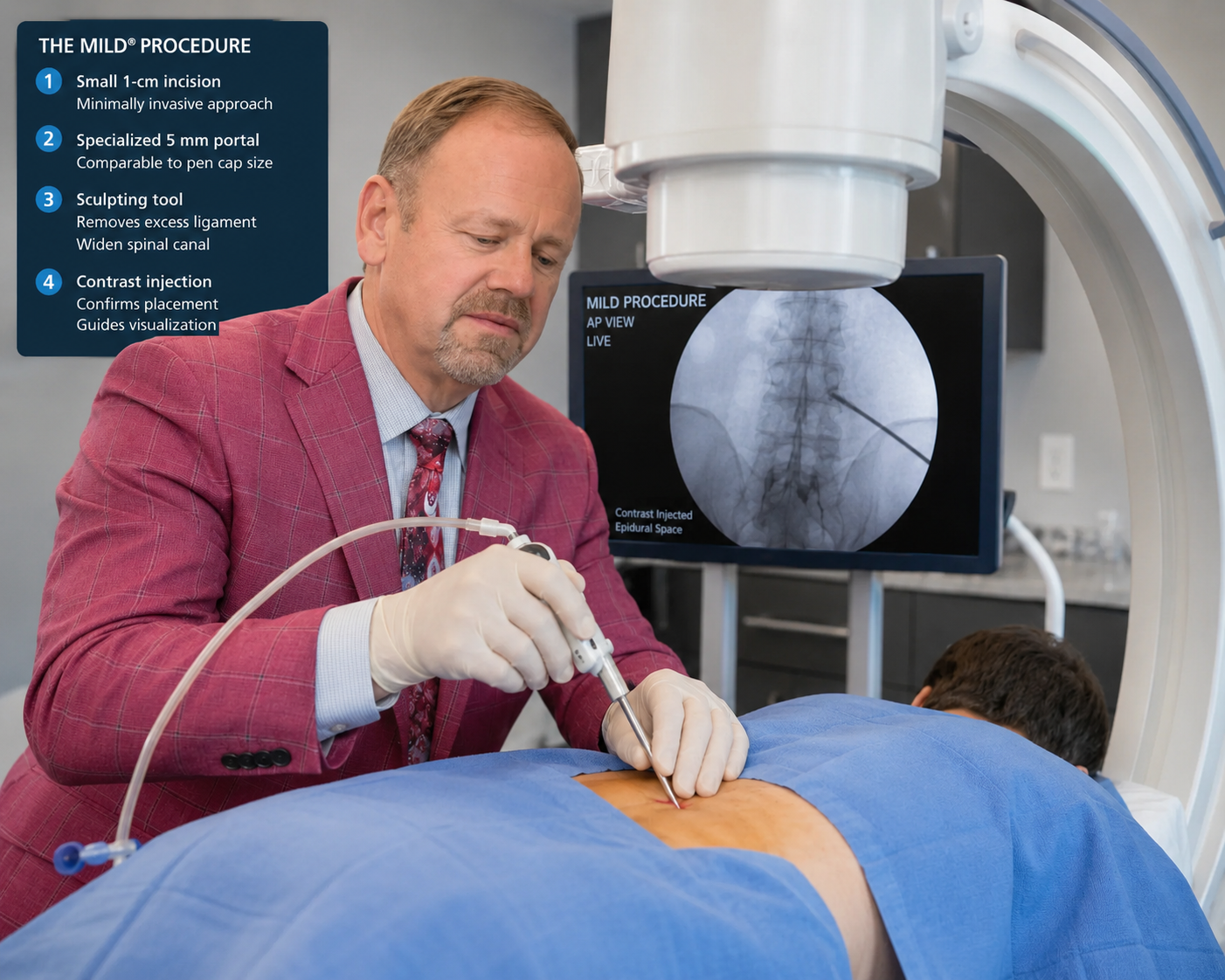
For a specific subset of patients — those whose lumbar spinal stenosis is being driven primarily by thickened ligamentum flavum — Aptiva Health offers the MILD procedure.
MILD is a minimally invasive, image-guided procedure performed through a small port (about the size of a pencil) under live X-ray guidance. The surgeon removes pieces of the thickened ligament and small bony elements that are crowding the spinal canal — restoring space for the nerves without making any incisions through muscle and without removing the full lamina.
Key features:
No general anesthesia — performed under local anesthesia and light sedation. Often a good option for older patients with cardiac, pulmonary, or surgical-risk concerns.
No stitches, no implants, no fusion.
Outpatient procedure — most patients go home within hours.
Quick recovery — most patients resume normal daily activity within days to weeks.
MILD does not work for every type of spinal stenosis — it is specifically designed for ligament-driven stenosis. Your surgeon will review your imaging to determine whether you are a candidate.
Step 5 — Minimally invasive decompression surgery
For patients whose stenosis is severe, whose symptoms have not responded to several months of conservative care, or whose anatomy clearly requires bony decompression, Aptiva Health's spine surgeons perform minimally invasive surgical decompression. The specific procedure depends on the location and pattern of the stenosis:
Laminectomy — removes the back portion of the vertebra (the lamina) to create more space around the compressed spinal cord or nerves. The most common surgery for symptomatic lumbar spinal stenosis.
Laminotomy — removes only a portion of the lamina, carving a window just large enough to relieve pressure in one specific spot. Used when stenosis is focal rather than diffuse.
Laminoplasty — performed on the cervical (neck) spine. Opens up the spinal canal by creating a hinge in the lamina rather than removing it, which preserves more of the spine's structure.
Minimally invasive spinal fusion (MAS® TLIF) — used when stenosis is combined with spinal instability or significant spondylolisthesis. The MAS® TLIF approach splits the back muscles rather than cutting them, which reduces blood loss, postoperative pain, scarring, and recovery time compared with traditional fusion.
Most Aptiva Health spinal stenosis surgeries are performed on an outpatient or short-stay basis. Recovery from laminectomy is typically four to six weeks before returning to non-strenuous activity and three months before full activity; recovery from a fusion is somewhat longer.

Why Choose Aptiva Health for Spinal Stenosis Treatment?
Many spinal stenosis patients end up coordinating care across three or four separate practices: a primary care office for the referral, a spine clinic for the evaluation, an imaging center for the MRI, a pain clinic for the injection, and a separate physical therapy practice for rehab. Aptiva Health is built differently. Every step happens under one roof:
Three board-certified orthopedic spine surgeons — Dr. Michael Casnellie, Dr. Jaideep Chunduri, and Dr. David McConda — all of whom specialize in minimally invasive spine surgery for stenosis.
A double board-certified pain management physician — Dr. Steven Ganzel — for fluoroscopy-guided epidural injections.
On-site digital X-ray and MRI at most locations, with same-week scheduling.
In-house physical therapy with therapists experienced in stenosis-specific flexion protocols and aquatic therapy.
The MILD procedure for patients who are candidates — a minimally invasive option performed without general anesthesia.
Same-day and walk-in spine appointments at most locations.
Free 24/7 virtual access to an Aptiva orthopedic provider via the HURT! app.
Transparent cash-pay pricing and broad in-network coverage — including Anthem, Aetna, Cigna, Humana, United Healthcare, Medicare, and most Medicaid plans.
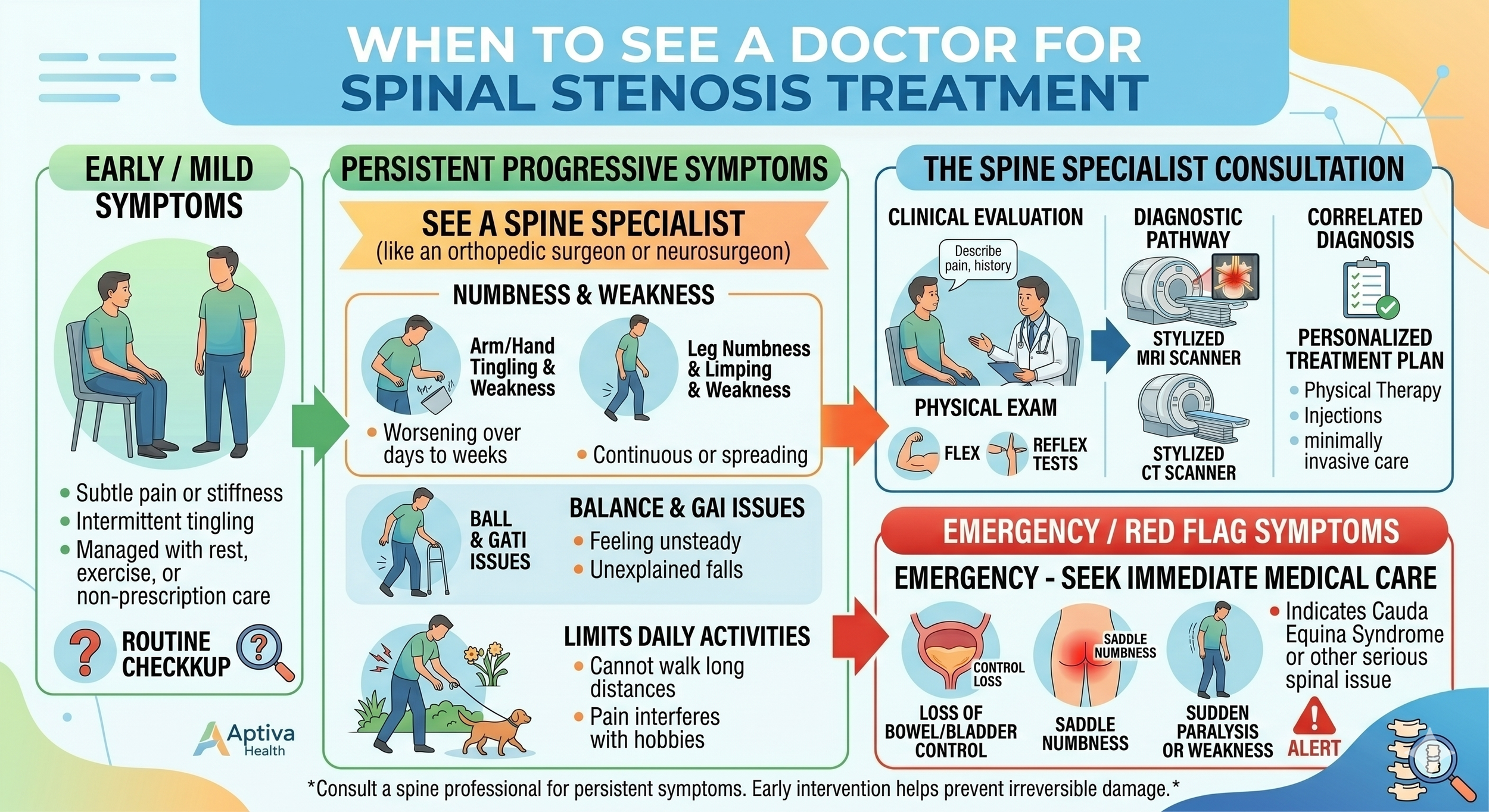
When Should You See a Doctor for Spinal Stenosis?
Most spinal stenosis comes on gradually, but certain patterns warrant prompt evaluation:
Leg pain or weakness that limits how far you can walk and is interfering with daily life.
Numbness, tingling, or weakness that is getting worse rather than staying stable.
Neck pain combined with hand clumsiness or balance problems — this can be a sign of cervical spinal stenosis affecting the spinal cord.
Symptoms that follow a fall or accident.
Get to an emergency room immediately if you experience: sudden loss of bladder or bowel control, sudden severe weakness in both legs, saddle anesthesia (numbness in the area that would touch a saddle), or sudden severe weakness or numbness in both arms. These can be signs of severe spinal cord or cauda equina compression, which is a surgical emergency.
For non-emergency spinal stenosis evaluation, Aptiva Health offers immediate spine appointments at most locations — so patients do not have to wait weeks or months for an evaluation.
Schedule your appointment today!

We Treat Spinal Stenosis Across Kentucky & Indiana!
Spine Center of Excellence: 3615 Newburg Road, Louisville, KY 40218
Louisville - East: 10100 Linn Station Road, Suite 1A, Louisville, KY 40223
Concussion & Sports Medicine Institute: 3611 Newburg Road, Louisville, KY 40218
Elizabethtown: 529 Westport Road, Suite 2, Elizabethtown, KY 42701
Indianapolis: 6801 Gray Road, Indianapolis, IN 46237
Louisville - Downtown: 300 South 13th Street, Louisville, KY 40203
Louisville - Middletown: 401 N English Station Road, Suite 1A, Louisville, KY 40223
Lexington Physical Therapy: 152 W Tiverton Way, Suite 180, Lexington, KY 40503
Mount Washington: 737 N Hwy 31e Byp, Suite 2, Mt. Washington, KY 40047
Northern Kentucky: 2093 Medical Arts Drive, Hebron, KY 41048
Frequently Asked Questions about Spinal Stenosis
Can you walk with spinal stenosis?
Yes, most patients with lumbar spinal stenosis can walk — but only for a limited distance before leg pain, weakness, or numbness forces them to stop. Many patients notice they can walk much farther while leaning on a shopping cart or walker, because bending forward opens the spinal canal slightly and takes pressure off the nerves. Walking ability often improves significantly with treatment.
What are the first signs of spinal stenosis?
The earliest signs of lumbar spinal stenosis are usually leg discomfort that comes on after standing or walking for a while and gets relieved by sitting down or leaning forward. Patients often notice they can walk a shorter distance before resting than they could a few years before. Numbness, tingling, or a sense that the legs are heavy on stairs are also common early signs.
Does spinal stenosis go away on its own?
No. Spinal stenosis is a structural narrowing of the spinal canal caused by gradual age-related changes, and the underlying narrowing does not reverse itself. However, the symptoms can vary significantly over time, and most patients can be managed effectively with physical therapy, anti-inflammatory medication, and epidural injections — without ever needing surgery.
What is the best treatment for spinal stenosis?
The best treatment depends on the severity of the stenosis, the specific symptoms, and the patient's overall health. Most patients respond well to a stepped-care approach: physical therapy and medication first, then targeted epidural injections, then minimally invasive options like the MILD procedure or laminectomy if conservative care is not enough. The right sequence is determined after a focused evaluation and MRI review.
Is spinal stenosis a disability?
Spinal stenosis can be disabling if it severely limits walking, standing, or working. The Social Security Administration recognizes spinal stenosis as a potentially qualifying condition for disability benefits under specific criteria (Listing 1.16) when the condition causes documented pseudoclaudication and significant limitations in walking. Many spinal stenosis patients, however, are able to remain fully active with appropriate treatment.
What is the MILD procedure for spinal stenosis?
The MILD procedure (Minimally Invasive Lumbar Decompression) is a same-day, image-guided procedure that removes pieces of thickened ligament and small bony elements crowding the spinal canal, creating more space for the nerves. It is performed under local anesthesia and light sedation through a port about the size of a pencil — no stitches, no implants, no fusion. MILD is specifically designed for patients whose stenosis is driven by thickened ligamentum flavum.
How long is recovery from a laminectomy?
Most patients are walking the day of laminectomy surgery. Return to non-strenuous work and driving typically takes four to six weeks. Return to full activity, including more demanding work and exercise, typically takes about three months. Aptiva's spine team coordinates post-operative physical therapy in-house, which speeds recovery and reduces the chance of recurrent symptoms.
What is the difference between spinal stenosis and a herniated disc?
A herniated disc is a specific injury where the soft inner material of a spinal disc bulges out through its outer wall and presses on a single nerve root, usually causing sharp one-sided leg pain (sciatica). Spinal stenosis is a more general narrowing of the spinal canal from age-related changes, often affecting multiple nerves at once and typically causing leg pain or weakness that worsens with standing and walking and improves with sitting or leaning forward.
Why does leaning forward relieve my back and leg pain?
Leaning forward — over a shopping cart, walker, kitchen counter, or stationary bike — physically opens the back of the spinal canal and the foramina where nerves exit the spine. In patients with lumbar spinal stenosis, this small change is often enough to relieve nerve compression and dramatically reduce pain. The "shopping cart sign" is one of the most reliable clinical clues for lumbar spinal stenosis.

The “Shopping Cart” Sign
What is neurogenic claudication?
Neurogenic claudication is the medical name for the classic symptom of lumbar spinal stenosis: leg pain, weakness, numbness, or heaviness that comes on with standing or walking and is relieved by sitting or leaning forward. It is caused by nerve compression in the spinal canal — not by reduced blood flow. The pattern is different from vascular claudication, which is caused by peripheral arterial disease and is relieved by simply stopping, not by changing position.
How quickly can I be seen at Aptiva Health for spinal stenosis?
Aptiva Health offers same-day and walk-in appointments for spine evaluations at most locations across Louisville, Lexington, Northern Kentucky, Elizabethtown, Mt. Washington, and Indianapolis. The HURT! app also provides free, 24/7 virtual access to an Aptiva orthopedic provider for after-hours guidance.
Stop guessing what's causing your back pain or leg pain. Aptiva Health's board-certified spine team can evaluate your symptoms, image the source of the pain, and start treatment — often within the same week.