Sacroiliac (SI) Joint Dysfunction

SI Joint Dysfunction
If you've been suffering with chronic lower back, buttock, hip, or groin pain — and the doctors and treatments you've tried haven't helped — your sacroiliac joint may be the source. The SI joint is responsible for an estimated 15 to 30 percent of chronic lower back pain, and it is one of the most commonly missed diagnoses in spine care because its pain pattern mimics a herniated disc, sciatica, hip pain, and piriformis syndrome. Many patients have been bouncing between providers for months or years before the correct diagnosis is finally made. Aptiva Health's coordinated spine team — interventional pain, surgical, and rehabilitation — finds the source of your back pain and builds a clear treatment plan, from physical therapy and diagnostic SI joint injections through radiofrequency ablation and, when needed, minimally invasive SI joint fusion in Louisville.
Medically reviewed by Michael Casnellie, MD, Jaideep Chunduri, MD, David McConda, MD, and Steven Ganzel, DO. Last reviewed: June 29, 2026.
Schedule your appointment today!
SI Joint Dysfunction — The Short Version
What it is: A condition where abnormal motion, alignment, inflammation, or arthritis of the sacroiliac joint produces chronic lower back, buttock, hip, or groin pain.
How common it is: Responsible for 15 to 30 percent of chronic lower back pain — and one of the most commonly missed diagnoses in spine care.
Where the pain is: Lower back below the belt line, the buttock, sometimes the back of the thigh — and almost never below the knee (a key feature that distinguishes it from sciatica).
What makes it worse: Sitting (especially in a car), getting up from sitting, rolling over in bed, climbing stairs, and standing on one leg.
How it's diagnosed: Provocative SI joint exam tests plus a fluoroscopy-guided diagnostic SI joint injection — the gold standard. Significant immediate pain relief after the injection confirms the SI joint as the pain generator.
Does it usually require surgery? No. About 90 percent of SI joint dysfunction responds to conservative care plus injections. Surgery — minimally invasive SI joint fusion — is reserved for patients who've failed appropriate non-surgical care.
What Is SI Joint Dysfunction?
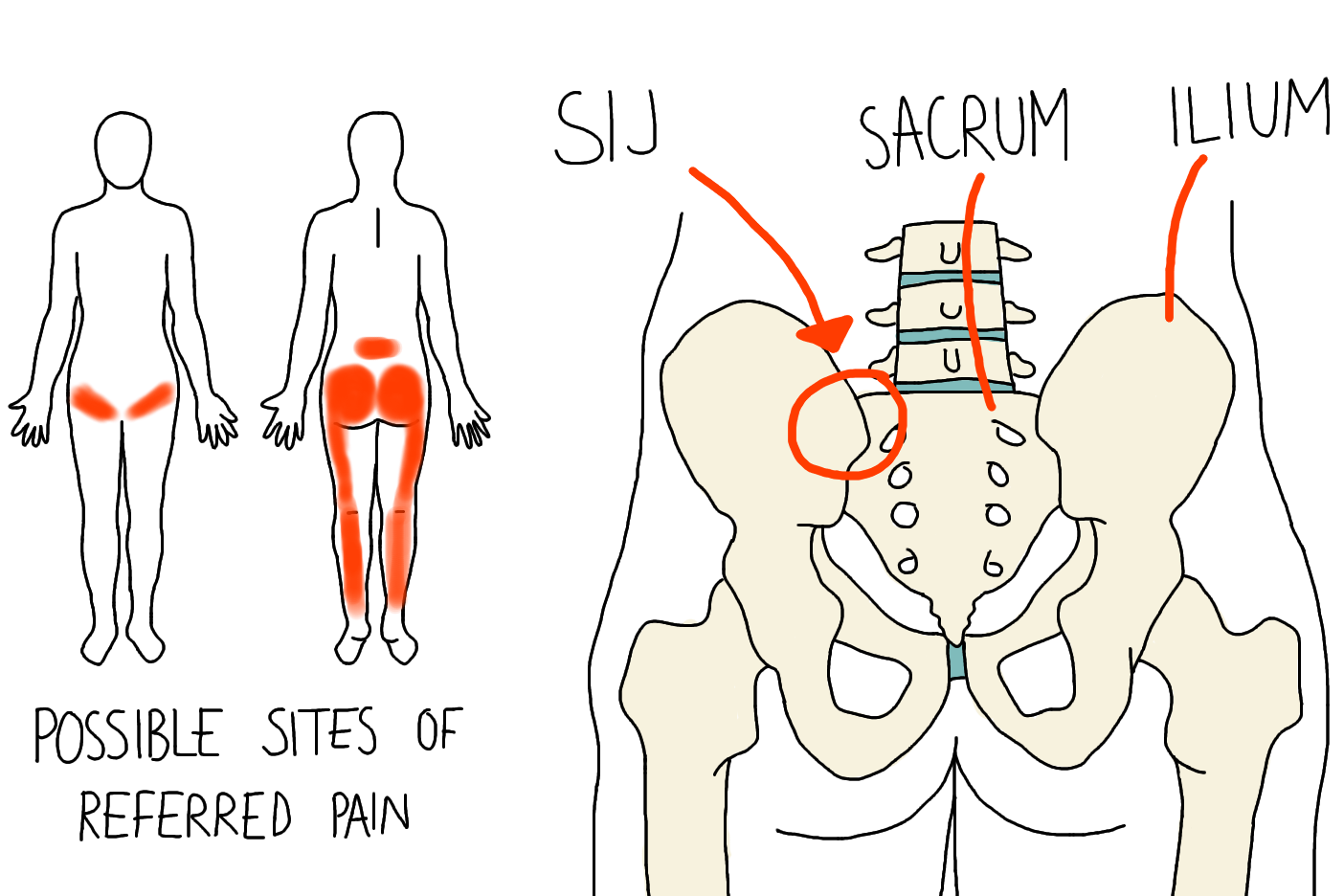
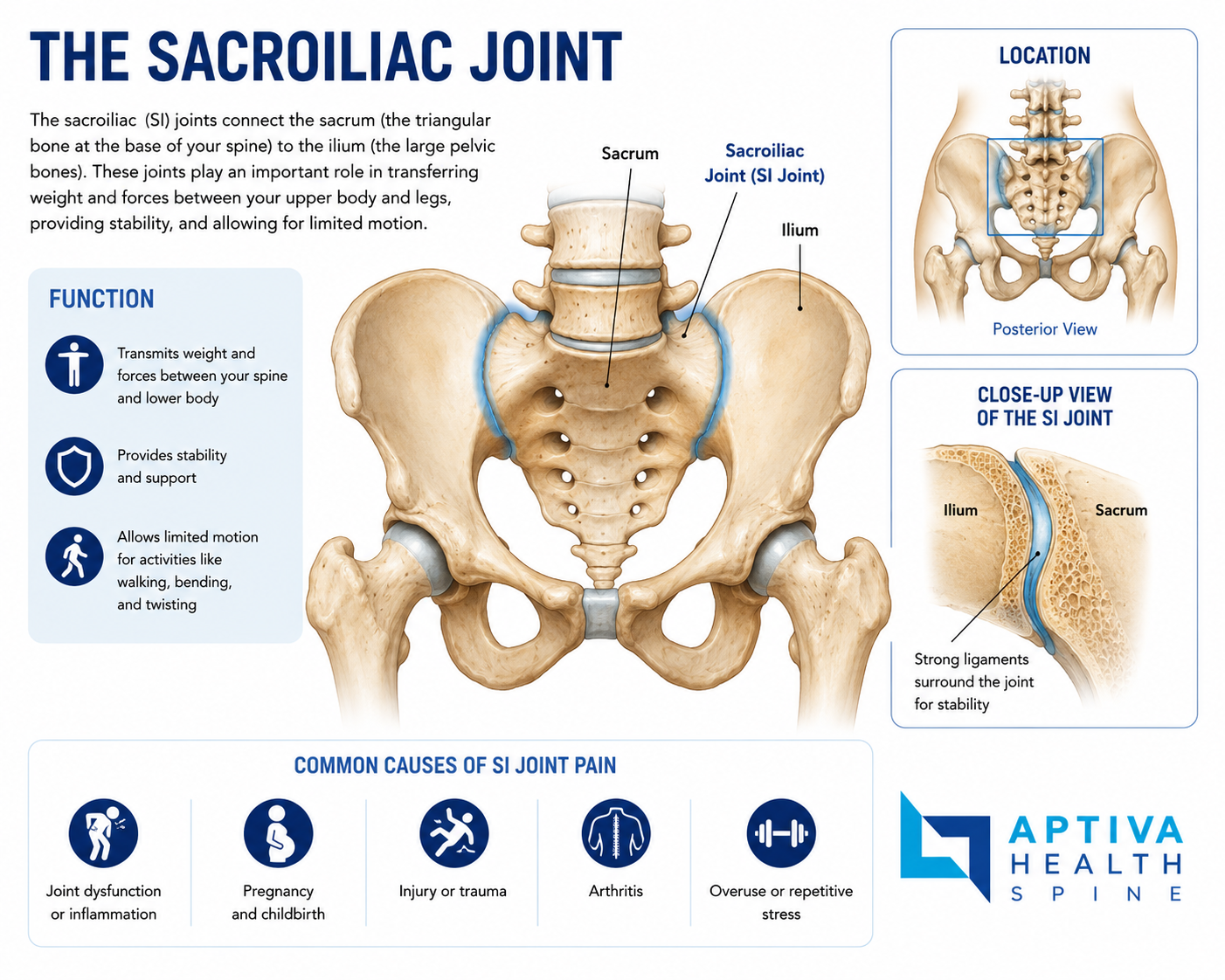
The sacroiliac (SI) joint is the strong, weight-bearing joint where the bottom of your spine — the sacrum — meets the back of your pelvis — the iliac bone. You have two of them, one on each side. Together, the two SI joints transfer the entire load of your upper body to your hips and legs every time you stand, walk, climb stairs, get out of a chair, or pick something up.
Unlike most joints, the SI joint is designed to have very little motion — typically just a few degrees. It's stabilized by some of the strongest ligaments in the body. But when something disrupts that delicate balance — trauma, arthritis, ligament laxity from pregnancy, increased mechanical stress after a lumbar fusion, or repetitive strain — the joint can become painful, dysfunctional, or unstable.
SI joint dysfunction is the umbrella term for any condition in which the SI joint is the source of pain. It can present as acute pain after a clear injury, or as chronic pain that develops slowly over years and gets misattributed to a herniated disc, sciatica, hip arthritis, or simply "lower back pain."
The pain pattern is typically focused in the lower back below the belt line and the buttock, often on one side more than the other. It may radiate to the back of the thigh but rarely below the knee — which is one of the most useful clinical clues distinguishing it from sciatica and disc-related radiculopathy.
Symptoms of SI Joint Dysfunction
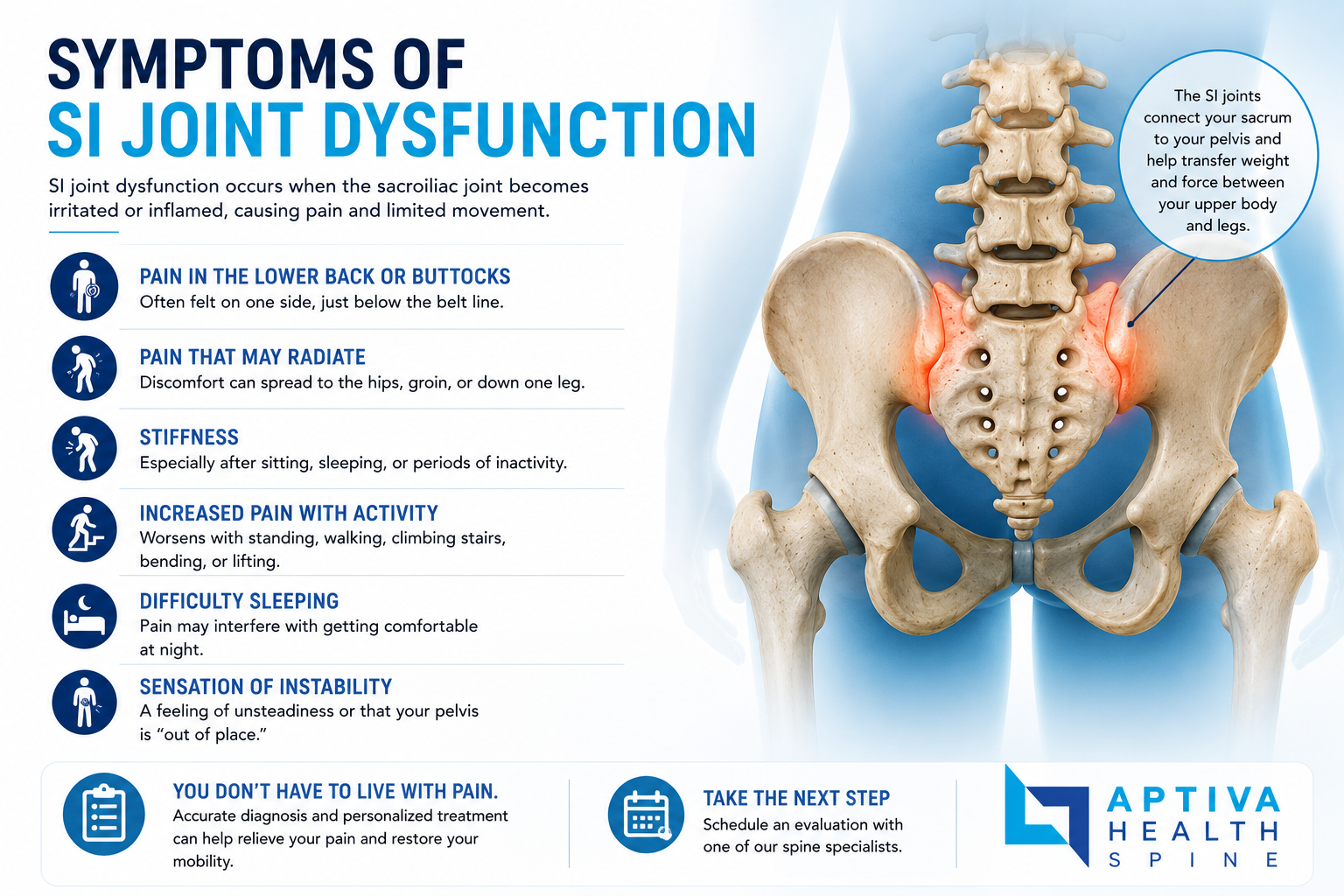
The symptoms of SI joint dysfunction are surprisingly specific once you know what to look for. The most common are:
Lower back pain below the belt line — the hallmark location
Buttock pain, often more on one side than the other
Pain radiating to the back of the thigh — but typically not below the knee
Hip or groin pain — many patients with SI joint dysfunction are initially evaluated for a hip problem
Pain with prolonged sitting — especially in a car or on a hard surface
Pain getting up from a chair or out of a car — often described as needing a moment to "straighten out"
Pain rolling over in bed — a very specific and common SI joint complaint
Pain climbing stairs
Pain standing on one leg — for example, while putting on pants
Sensation that the lower back or pelvis is "giving way" or unstable
Stiffness after sitting for a while or in the morning after sleeping
The Fortin Finger Test
If someone with chronic lower back pain can point to the source of their pain with one finger — and that finger lands directly over the dimple at the back of the pelvis (the posterior superior iliac spine) — the SI joint is highly likely to be involved. This is called the Fortin finger test and is one of the most useful pieces of physical exam evidence in SI joint diagnosis.
What Causes SI Joint Dysfunction?
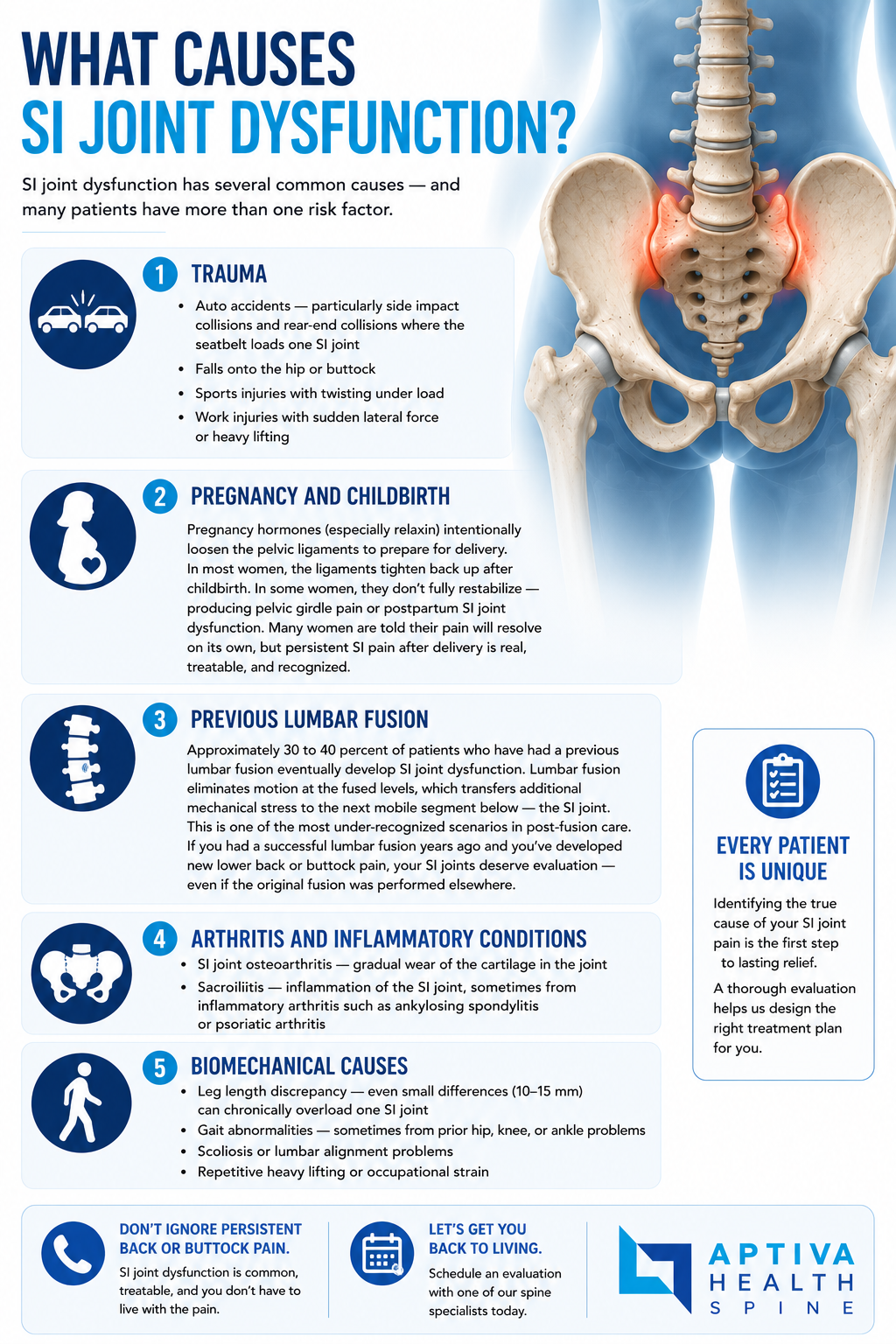
SI joint dysfunction has several common causes — and many patients have more than one risk factor.
Trauma
Auto accidents — particularly side impact collisions and rear-end collisions where the seatbelt loads one SI joint
Falls onto the hip or buttock
Sports injuries with twisting under load
Work injuries with sudden lateral force or heavy lifting
Pregnancy and Childbirth
Pregnancy hormones (especially relaxin) intentionally loosen the pelvic ligaments to prepare for delivery. In most women, the ligaments tighten back up after childbirth. In some women, they don't fully restabilize — producing pelvic girdle pain or postpartum SI joint dysfunction. Many women are told their pain will resolve on its own, but persistent SI pain after delivery is real, treatable, and recognized.
Previous Lumbar Fusion
Approximately 30 to 40 percent of patients who have had a previous lumbar fusion eventually develop SI joint dysfunction. Lumbar fusion eliminates motion at the fused levels, which transfers additional mechanical stress to the next mobile segment below — the SI joint. This is one of the most under-recognized scenarios in post-fusion care. If you had a successful lumbar fusion years ago and you've developed new lower back or buttock pain, your SI joints deserve evaluation — even if the original fusion was performed elsewhere.
Arthritis and Inflammatory Conditions
SI joint osteoarthritis — gradual wear of the cartilage in the joint
Sacroiliitis — inflammation of the SI joint, sometimes from inflammatory arthritis such as ankylosing spondylitis or psoriatic arthritis
Biomechanical Causes
Leg length discrepancy — even small differences (10-15 mm) can chronically overload one SI joint
Gait abnormalities — sometimes from prior hip, knee, or ankle problems
Scoliosis or lumbar alignment problems
Repetitive heavy lifting or occupational strain
How Is SI Joint Dysfunction Diagnosed?
This is where the SI joint story is different from most spine conditions. Because SI joint pain mimics so many other problems, accurate diagnosis requires a structured pathway — and it's the diagnosis itself, not the treatment, that's often the hardest part.
Step 1: Focused History
Your provider will ask about:
The exact location of your pain (the Fortin finger test is part of this)
What makes it better and worse (sitting, getting up, rolling over)
Whether the pain radiates above or below the knee
Whether you've had a fall, auto accident, pregnancy, or prior lumbar fusion
How long you've had the pain and what treatments have already been tried
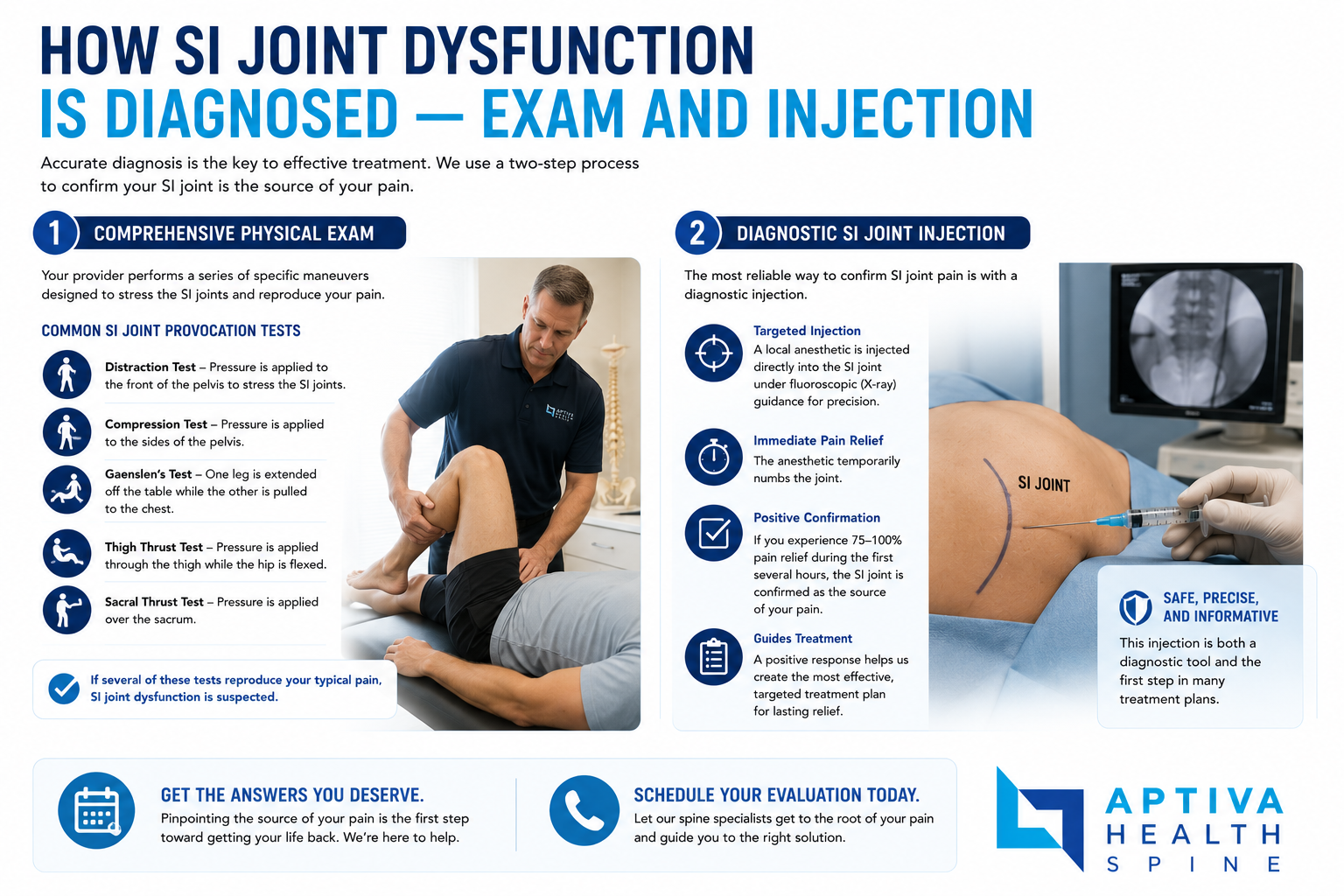
Step 2: Provocative SI Joint Examination
A focused physical exam uses five provocative SI joint tests:
Patrick or FABER test — flexion, abduction, and external rotation of the hip
Gaenslen test — extending one hip while flexing the opposite hip
Thigh thrust — posterior pressure through the femur
Distraction — opening the front of the SI joint
Compression — squeezing the pelvis together
At least three of five positive tests is considered diagnostic for SI joint involvement — a well-validated benchmark from the spine literature.
Step 3: Imaging
X-ray — rules out fracture, evaluates alignment, screens for arthritis
MRI of the lumbar spine — rules out lumbar disc and stenosis as the cause
CT or MRI of the SI joints — assesses bony anatomy, inflammation, or sacroiliitis
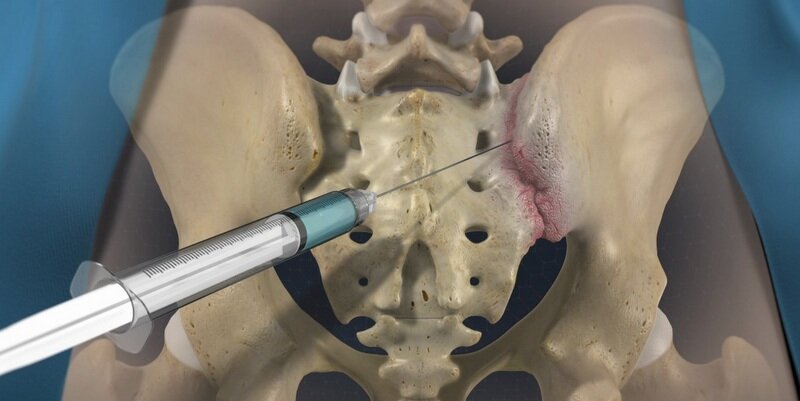
Step 4: Diagnostic SI Joint Injection — The Gold Standard
The single most important test for confirming SI joint pain is a fluoroscopy-guided diagnostic SI joint injection. Dr. Steven Ganzel, our interventional pain specialist, places a small amount of local anesthetic directly into the SI joint under live X-ray guidance. If your pain is significantly relieved (typically at least 50 to 75 percent) immediately after the injection, the SI joint is confirmed as the pain generator.
Many surgeons require two confirmatory diagnostic injections before considering surgical fusion to ensure the diagnosis is correct.
This diagnostic precision is why patients who've been bouncing between providers for months or years often finally get a clear answer at Aptiva.
Schedule your appointment today!
SI joint pain vs. sciatica vs. low back pain - how to tell the difference
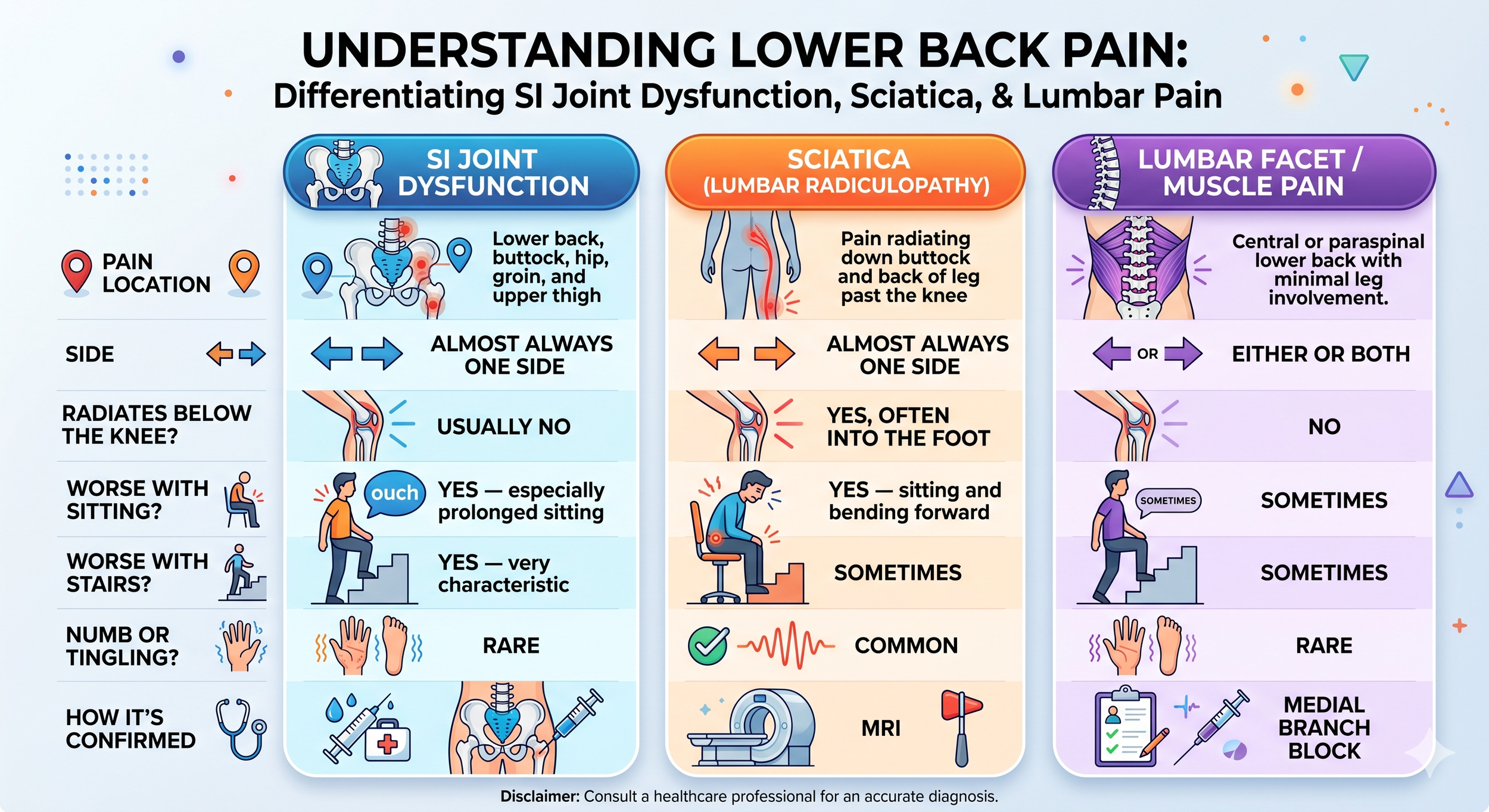
The most common reason SI joint dysfunction goes untreated for years is that patients and providers mistake it for sciatica or general lumbar back pain. Here is how the patterns typically differ.
SI joint dysfunction typically has a pain location in the lower back, buttock, hip, or occasionally groin or upper thigh that is almost always on one side. There is typically no radiating pain. It is typically made worse by prolonged sitting or climbing stairs and rarely creates numbness or tingling in the leg. It is confirmed by a diagnostic SI joint injection.
Sciatica (lumbar radiculopathy) is typically located in the lower back radiating down the buttock and back of the leg, often past the knee. It’s almost always on one side and can radiate into the foot. It is made worse by sitting and bending forward and sometimes with climbing stairs. It is often accompanied by numbness or tingling in the leg and is confirmed with an MRI and medical examination.
Lumbar facet or muscle pain is often centrally located or paraspinal in the lower back with minimal leg involvement. It can be on either or both sides and does not radiate below the knee. It can sometimes be made worse with sitting and climbing stairs but rarely is accompanied by numbness or tingling in the leg. It is confirmed by a medical examination and medial branch block if the facet joint is involved.
Many patients have more than one source of pain — for example, both SI joint dysfunction and a herniated disc — which is why a thorough evaluation by a fellowship-trained spine team is the most reliable way to identify everything contributing to your pain.

Treatment Options for SI Joint Dysfunction
Aptiva Health treats SI joint dysfunction with a stepped-care approach. Most patients get significant relief from non-surgical care; the patients who do not respond after several months of high-quality conservative treatment are candidates for SI joint fusion. If you have been diagnosed with SI joint dysfunction, which can lead to one or both of the SI joints becoming painful, your doctor will first recommend exploring conservative treatment options.
STEP 1 EARLY TREATMENTS
Medications may include:
Analgesics and NSAIDS
Opioid medications prescribed by a physician (opioids should be used only for a short period of time and under a physician’s supervision, as opioids can be addictive, aggravate depression, and have other side effects)
Anticonvulsants—prescribed drugs primarily used to treat seizures—may be useful in treating people with sciatica
Antidepressants such as tricyclics and serotonin, and norepinephrine reuptake inhibitors have been commonly prescribed for chronic low back pain (prescribed by a physician)
Self-management:
Hot or cold packs
Resuming normal activities as soon as possible may ease pain; bed rest is not recommended
Exercises that strengthen core or abdominal muscles may help to speed recovery from chronic low back pain. Always check first with a physician before starting an exercise program and to get a list of helpful exercises.
STEP 2 Additional CONSERVATIVE TREATMENT OPTIONS:
Transcutaneous electrical nerve stimulation (TENS) involves wearing a battery-powered device which places electrodes on the skin over the painful area that generate electrical impulses designed to block or modify the perception of pain
Physical therapy programs to strengthen core muscle groups that support the low back, improve mobility and flexibility, and promote proper positioning and posture are often used in combination with other interventions
Spinal manipulation and spinal mobilization are approaches in which doctors of chiropractic care use their hands to mobilize, adjust, massage, or stimulate the spine and the surrounding tissues. Manipulation involves a rapid movement over which the individual has no control; mobilization involves slower adjustment movements. The techniques may provide small to moderate short-term benefits in people with chronic low back pain but neither technique is appropriate when a person has an underlying medical cause for the back pain such as osteoporosis, spinal cord compression, or arthritis.
Traction involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction but the back pain tends to return once the traction is released.
Dry needling is moderately effective for chronic low back pain. It involves inserting thin needles into precise points throughout the body and stimulating them (by twisting or passing a low-voltage electrical current through them), which may cause the body to release naturally occurring painkilling chemicals such as endorphins, serotonin, and acetylcholine.
Behavioral approaches include:
Biofeedback involves attaching electrodes to the skin and using an electromyography machine that allows people to become aware of and control their breathing, muscle tension, heart rate, and skin temperature; people regulate their response to pain by using relaxation techniques
Cognitive therapy involves using relaxation and coping techniques to ease back pain
STEP 3 INJECTION THERAPY OPTIONS:
Interventional pain management injections to include:
SI Joint Injections. Sacroiliac (SI) joint pain is easily confused with back pain from the spine. Sometimes injecting the SI joint with lidocaine may help your doctor determine whether the SI joint is the source of your pain. If the joint is injected and your pain does not go away, it may be coming from a different source. During the procedure, a mixture of local anesthetic and steroid is injected into the SI joint. The local anesthetic will numb the area, and steroid may help lower the swelling. The steroid should reduce the pain and improve the motion in your hip or buttock.

Medial branch blocks injection used to determine if the facet joint is causing the patient's back pain. Facet joints are pairs of small joints between the vertebrae in the back of the spine.
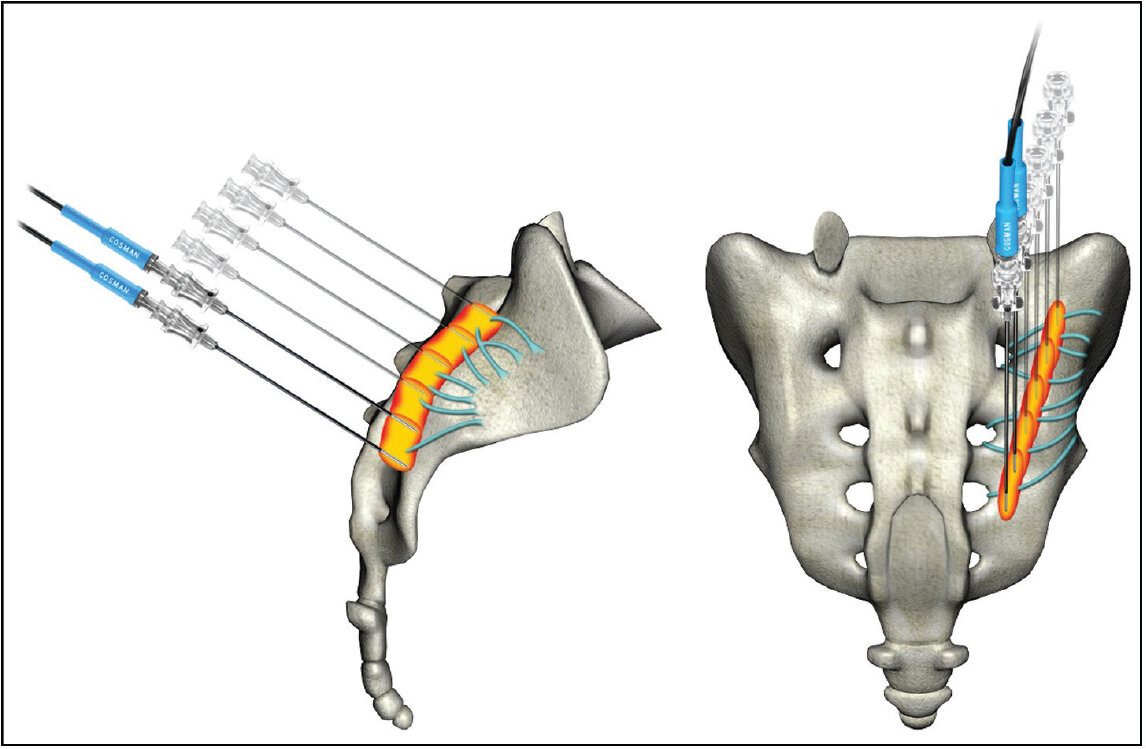
Radiofrequency ablation involves inserting a fine needle into the area causing the pain through which an electrode is passed and heated to destroy nerve fibers that carry pain signals to the brain. Also called a rhizotomy, the procedure can relieve pain for several months.

STEP 4 minimally invasive si joint fusion
SI joint fusion is the surgical treatment for SI joint dysfunction that has not responded to several months of conservative care. The procedure stabilizes the joint by fusing the sacrum and ilium together, eliminating the abnormal motion that causes pain.
Aptiva Health's board-certified orthopedic spine surgeons Dr. Michael Casnellie, Dr. Jaideep Chunduri and Dr. David McConda perform minimally invasive SI joint fusion through a small incision on the side of the buttock. Specialized titanium implants are placed across the joint under live X-ray and navigation guidance, locking the joint in proper alignment and allowing bone to grow across it over the following months.
Compared with traditional open SI joint fusion, the minimally invasive approach offers:
A smaller incision (typically 1 to 1.5 inches).
Less blood loss and less surgical trauma.
A shorter procedure — most cases are completed in about an hour.
Outpatient or short-stay surgery — most patients go home the same day or the next morning.
Faster return to non-strenuous activity — typically two to four weeks.
High patient satisfaction rates in published studies (around 80 to 90 percent of properly selected patients report significant pain relief).
step 5 recovery after si joint fusion
Recovery after minimally invasive SI joint fusion happens in stages. Specifics vary by patient, but a typical timeline at Aptiva Health is:
Week 1: Walking with a walker or cane is encouraged starting the day of surgery. Pain is managed with a multimodal regimen designed to minimize opioid use.
Weeks 2 to 4: Most patients transition off assistive devices and resume desk-based work. Driving usually resumes around week three to four.
Weeks 4 to 12: Structured physical therapy with Aptiva's in-house team focuses on restoring hip and pelvic mobility, building core and gluteal strength, and gradually returning to normal activities.
Months 3 to 6: Bone fusion progresses across the joint. Most patients return to full, unrestricted activity by three months.
Month 6 and beyond: Solid bony fusion is typically achieved. Long-term outcomes from the minimally invasive technique are excellent and have been documented in multiple peer-reviewed studies.

Why Choose Aptiva Health for Your SI Joint Care
The diagnosis is the hard part — and we do it well. SI joint dysfunction is famously misdiagnosed because its pain pattern mimics so many other conditions. Aptiva's structured diagnostic pathway — focused history, five provocative SI joint exam tests, MRI to rule out other causes, and fluoroscopy-guided diagnostic SI joint injection — gets to a clear answer when other providers have not. Many patients who've been bouncing between providers for months or years finally get their diagnosis here.
A surgeon who teaches this procedure nationally. Dr. David McConda is fellowship-trained at OrthoCarolina Spine Center through the AOSpine North America Spine Surgery Fellowship and serves as AOSpine course faculty teaching minimally invasive SI joint fusion technique to other surgeons. When SI joint fusion is the right answer at Aptiva, you're being treated by a surgeon who trains other surgeons in this exact procedure.
Three SI joint fusion surgeons across our footprint. Dr. McConda (Louisville), Dr. Michael Casnellie (Louisville, treating spine patients since 2005), and Dr. Jaideep Chunduri (Northern Kentucky / Cincinnati, 20+ years and nationally recognized for minimally invasive spine technique) each perform minimally invasive SI joint fusion. Dr. Chunduri holds active medical licenses in both Kentucky and Ohio, which makes him a uniquely accessible option for cross-border patients from the Greater Cincinnati metro.
Conservative care first. About 90 percent of SI joint dysfunction responds to conservative care plus interventional pain procedures. We don't push surgery. We work through the treatment ladder — physical therapy, SI joint injections, radiofrequency ablation — and reserve SI joint fusion for patients who've truly exhausted non-surgical options.
A complete continuum under one roof. From your first evaluation to MRI, diagnostic injection, physical therapy, RFA, and surgery if needed — Aptiva offers the complete spine and SI joint care continuum so you don't get bounced between unrelated providers and facilities.
Same-day and walk-in appointments. Stop waiting weeks for an answer. Most patients see an Aptiva spine provider within days of calling.
Post-fusion SI joint expertise. If you've had a previous lumbar fusion and developed new lower back or buttock pain, our team is experienced in recognizing and treating adjacent-segment SI joint dysfunction — including patients whose original fusion was performed elsewhere.
Postpartum SI joint care. Pelvic girdle pain that persists after pregnancy is real, treatable, and worth evaluating. We see and treat postpartum SI joint dysfunction every week.
Transparent insurance and cash-pay pricing. We accept most major insurance, Medicare, Medicaid Managed Care, workers' compensation, and auto insurance (PIP and Medpay). For self-pay patients, transparent bundled pricing and affordable cash-pay MRI are available.
Documentation that supports your case. For SI joint injuries from work or auto accidents, our team works directly with employers, adjusters, and attorneys on documentation and coordination of care.
Schedule your appointment today!
Your Aptiva Health Spine Care Team
At Aptiva Health, your SI joint care is delivered by a coordinated multidisciplinary team — interventional pain, surgical, and rehabilitation — that focuses exclusively on conditions of the spine and SI joint.

Interventional Pain
Dr. Steven Ganzel, DO — Double board-certified in Physical Medicine & Rehabilitation and Interventional Pain Management. Performs the full range of fluoroscopy-guided SI joint procedures including diagnostic SI joint injections, therapeutic corticosteroid SI joint injections, SI joint radiofrequency ablation, and medial branch blocks. Most patients begin their SI joint care with Dr. Ganzel for diagnosis and conservative interventional management.

Orthopedic Spine Surgeons
Dr. Michael Casnellie — Board-certified orthopedic spine surgeon treating spine patients in Louisville since 2005. Performed Kentucky's first Prestige cervical artificial disc replacement.

Dr. David McConda — Board-certified orthopedic spine surgeon; fellowship-trained at OrthoCarolina Spine Center through the AOSpine North America Spine Surgery Fellowship.

Dr. Jaideep Chunduri — Board-certified orthopedic spine surgeon with more than 20 years of clinical experience in the Greater Cincinnati and Northern Kentucky region. Nationally recognized for his patient care approach and minimally invasive spinal surgery techniques. Performs the full range of cervical and lumbar spine procedures including minimally invasive disc replacement, microdiscectomy, sacroiliac joint fusion, and complex revision surgery.
Advanced Practice Providers
Kayla Troutman, PA-C — Orthopedic physician assistant
David Koonce, DNP — Doctor of Nursing Practice
Michael Gilbert, PA-C — Orthopedic physician assistant
Bradley Stephenson, PA-C — Orthopedic physician assistant
Physical Therapy & Imaging
Aptiva's orthopedic physical therapy team includes therapists experienced in SI joint stabilization and pelvic biomechanics. On-site imaging including X-ray, MRI, and CT is integrated with the spine team so evaluation, imaging, diagnostic injection, and treatment all happen under one roof.

Where We Treat SI Joint Dysfunction
Aptiva Health treats SI joint dysfunction across our network of locations in Kentucky and Indiana. One call connects you to any of our locations: 1-844-999-3627 (DOCS).
Louisville Metro
Aptiva Health — Louisville East — 10100 Linn Station Road, Suite 1A, Louisville, KY 40223
Aptiva Health — Louisville Downtown — 300 South 13th Street, Louisville, KY 40203
Aptiva Health — Louisville Middletown — 401 N English Station Road, Suite 1A, Louisville, KY 40223
Aptiva Health Imaging (Louisville) — 3615 Newburg Road, Suite 106, Louisville, KY 40218
Concussion & Sports Medicine Institute — 3611 Newburg Road, Louisville, KY 40218
South of Louisville
Lexington / Central Kentucky
Aptiva Health — Lexington — 230 Fountain Court, Suite 180, Lexington, KY 40509
Aptiva Health Lexington MRI — 426 Codell Drive, Lexington, KY 40509
Aptiva Health Lexington Physical Therapy — 152 W Tiverton Way, Suite 180, Lexington, KY 40503
Northern Kentucky / Cincinnati Metro
Indianapolis
Main scheduling line for all locations: 1-844-999-3627 (DOCS)
SI Joint Dysfunction: Frequently Asked Questions
What is SI joint dysfunction?
Sacroiliac (SI) joint dysfunction is a condition in which abnormal motion, alignment, inflammation, or arthritis of the sacroiliac joint produces chronic lower back, buttock, hip, or groin pain. The SI joint is the strong, weight-bearing joint where the bottom of your spine (the sacrum) meets the back of your pelvis (the iliac bone) — you have two of them, one on each side. SI joint dysfunction is responsible for an estimated 15 to 30 percent of chronic lower back pain and is one of the most commonly missed diagnoses in spine care because its pain pattern mimics lumbar disc pain, sciatica, hip pain, and piriformis syndrome.
What are the symptoms of SI joint dysfunction?
The most common symptoms include lower back pain (typically below the belt line), buttock pain that is often one-sided, pain radiating to the back of the thigh (rarely below the knee), pain with prolonged sitting (especially in a car or on a hard surface), pain getting up from a chair or out of a car, pain rolling over in bed, pain climbing stairs, pain standing on one leg, and a sensation that the lower back or pelvis is giving way. Many patients describe the pain as worse on one side than the other.
What causes SI joint dysfunction?
SI joint dysfunction has several common causes. Trauma — particularly auto accidents and falls onto the hip or buttock — is one of the most common acute causes. Pregnancy and childbirth loosen the pelvic ligaments and sometimes the SI joint does not fully restabilize after delivery. Previous lumbar fusion surgery transfers additional mechanical stress to the SI joint; approximately 30 to 40 percent of post-fusion patients eventually develop SI joint dysfunction. Other causes include repetitive heavy lifting or occupational strain, leg length discrepancy, gait abnormalities, SI joint arthritis, and inflammatory arthritis such as ankylosing spondylitis or psoriatic arthritis.
How is SI joint dysfunction diagnosed?
SI joint dysfunction is diagnosed through a combination of focused history, physical examination, and confirmatory injection. The history identifies the pain location and what makes it worse. The physical exam includes provocative SI joint tests — Patrick or FABER, Gaenslen, thigh thrust, distraction, and compression — and at least three of five positive tests is considered diagnostic. MRI or CT is obtained to rule out other causes. The gold standard for confirming the diagnosis is a fluoroscopy-guided diagnostic SI joint injection of local anesthetic: significant pain relief immediately after the injection confirms the SI joint as the pain generator.
What is the difference between SI joint pain and sciatica or a herniated disc?
All three can cause lower back pain that radiates into the buttock or leg, which is why SI joint dysfunction is so commonly misdiagnosed. The key differences: SI joint pain typically stays in the lower back and buttock with possible radiation to the back of the thigh, but rarely radiates below the knee — and pain is reproduced by provocative SI joint tests. Sciatica from a herniated lumbar disc typically causes sharp, electric, burning pain that radiates all the way down the leg below the knee — often to the foot — and is reproduced by nerve tension tests like the straight leg raise. Distinguishing them requires a careful exam and often diagnostic injection.
Can SI joint dysfunction develop after a lumbar fusion?
Yes — and it is very common. Approximately 30 to 40 percent of patients who have had a previous lumbar fusion will eventually develop SI joint dysfunction. This is because lumbar fusion eliminates motion at the fused spinal levels, which transfers additional mechanical stress to the next mobile segment below the fusion — the SI joint. Patients who had a successful lumbar fusion years ago and then develop new lower back or buttock pain should be evaluated for SI joint dysfunction, including patients whose original fusion was performed elsewhere.
Why does my SI joint hurt during or after pregnancy?
Pregnancy produces relaxin and other hormones that intentionally loosen the pelvic ligaments — including the strong ligaments that stabilize the SI joints — to prepare for childbirth. In most women, the ligaments tighten back up after delivery. In some women, they don't fully restabilize, leaving the SI joint loose and painful. This is sometimes called pelvic girdle pain or postpartum SI joint dysfunction. Persistent pain beyond several months after delivery deserves orthopedic evaluation — pelvic girdle pain is real, treatable, and recognized by modern spine care.
What is the treatment for SI joint dysfunction?
Most SI joint dysfunction is treated conservatively, with a stepwise approach. First-line treatment includes physical therapy focused on SI joint stabilization, hip strengthening, and core strengthening; anti-inflammatory medication; activity modification; and sometimes an SI joint belt. When conservative care isn't enough, interventional pain procedures provide both diagnosis and treatment: a fluoroscopy-guided SI joint injection of corticosteroid often provides lasting relief, and SI joint radiofrequency ablation (lateral branch RFA) can extend that relief by months or years. When conservative and interventional care has failed and the SI joint has been confirmed as the pain generator, minimally invasive SI joint fusion is the surgical option.
Do I need surgery for SI joint dysfunction?
Most patients with SI joint dysfunction do not need surgery. Approximately 90 percent respond to a structured course of physical therapy, anti-inflammatory medication, activity modification, and interventional pain procedures (SI joint injections and radiofrequency ablation). Surgery — minimally invasive SI joint fusion — is generally considered only when conservative care has failed after at least six months, the SI joint has been confirmed as the pain generator with one or two positive diagnostic injections, and the patient's quality of life is significantly impacted.
Who treats SI joint dysfunction at Aptiva Health?
SI joint dysfunction at Aptiva Health is managed by a coordinated spine team. Dr. Steven Ganzel, our interventional pain physician, performs diagnostic and therapeutic SI joint injections and SI joint radiofrequency ablation. Three board-certified orthopedic spine surgeons perform minimally invasive SI joint fusion when surgery is the right answer: Dr. David McConda, fellowship-trained at OrthoCarolina Spine Center through the AOSpine North America Spine Surgery Fellowship; Dr. Michael Casnellie, treating spine patients in Louisville since 2005; and Dr. Jaideep Chunduri, nationally recognized for minimally invasive spinal surgery with more than 20 years of practice in the Greater Cincinnati and Northern Kentucky region. Advanced practice providers Kayla Troutman PA-C, David Koonce DNP, Michael Gilbert PA-C, and Bradley Stephenson PA-C support evaluation, pre- and post-operative care, and follow-up.
When should I see a doctor for SI joint pain?
You should see a doctor for lower back and buttock pain that has persisted more than two to four weeks without improvement, new back pain that developed after a fall, auto accident, pregnancy, or previous lumbar fusion, pain that interferes with sleep, work, or daily activities, or pain that has been attributed to other diagnoses (such as a 'pulled muscle' or 'pinched nerve') without improvement after appropriate treatment. SI joint dysfunction is commonly missed in primary care and even in some specialty settings — if you've been treated for a lumbar disc problem or sciatica without improvement, the SI joint is worth evaluating.
Where can I get SI joint treatment near me?
Aptiva Health treats SI joint dysfunction at our locations across Kentucky and Indiana, including Louisville (Central, East, Downtown, and Middletown), Elizabethtown, Mount Washington, Lexington, Northern Kentucky (Hebron), and Indianapolis. Our spine team includes three board-certified orthopedic spine surgeons (Dr. Michael Casnellie, Dr. Jaideep Chunduri, and Dr. David McConda), an interventional pain physician (Dr. Steven Ganzel) who performs all SI joint diagnostic and therapeutic procedures, physical therapists, and advanced practice providers. Call 1-844-999-3627 (DOCS) to schedule an evaluation at the location nearest you.
Sources: Mayo Clinic, Johns Hopkins Medicine, AAOS OrthoInfo, and American Family Physician.
Videos About SI Joint Dysfunction
Hear from Lorie in the video below about her SI-joint fusion with Dr. Casnellie!
Learn more about SI-joint fusions with Dr. David McConda!

Studies show that the SI joint is a source of pain in 15-30% of patients with chronic low back pain. Does this include you?
For more information: